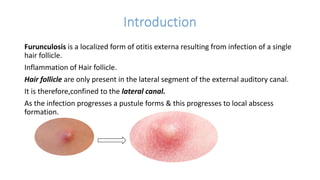
This document discusses furunculosis, a localized infection of the external auditory canal caused by infection of a hair follicle. It presents risk factors like allergies and diabetes, signs and symptoms of pain and discharge, and management through topical and oral antibiotics as well as incision and drainage if an abscess forms. Without treatment, the infection can spread and cause scarring of the ear canal. Patient education focuses on warm compresses and hand washing to prevent spread.