Downloaded 968 times
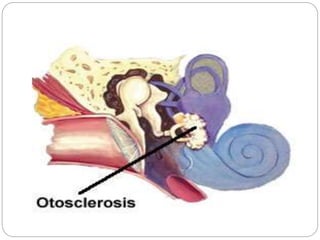


Otosclerosis is a condition where abnormal bone growth occurs in the middle ear, usually affecting both ears. This causes the stapes bone to become fixed, preventing sound vibrations from being transmitted effectively and resulting in conductive hearing loss. It is classified based on histological and clinical presentations. Diagnosis involves tests like audiometry and imaging. Treatment options range from hearing aids for mild cases to stapedectomy surgery to restore hearing by replacing or drilling the stapes bone.














































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)







