Download to read offline
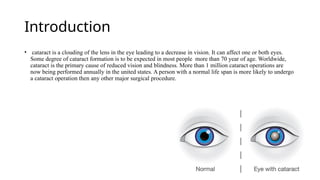


cataract is a clouding of the lens in the eye leading to a decrease in vision. It can affect one or both eyes. Some degree of cataract formation is to be expected in most people more than 70 year of age. Worldwide, cataract is the primary cause of reduced vision and blindness. More than 1 million cataract operations are now being performed annually in the united states. A person with a normal life span is more likely to undergo a cataract operation then any other major surgical procedure.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














