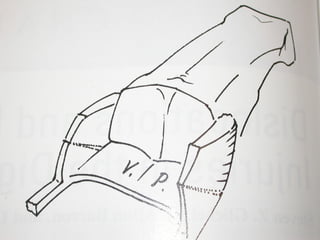
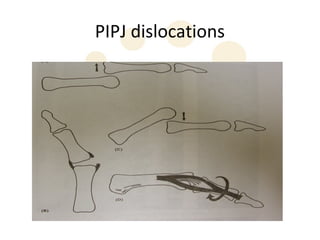
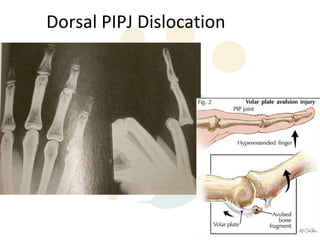
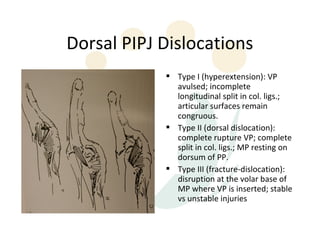
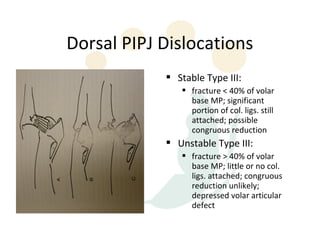
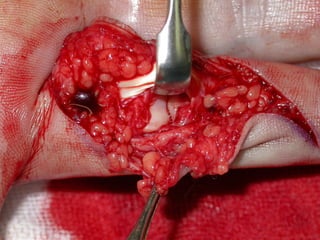
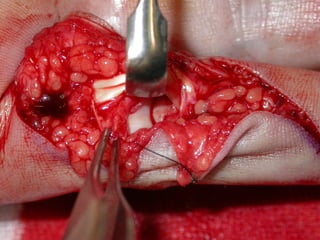
The proximal interphalangeal joint (PIPJ) is stabilized by bony articulations, collateral ligaments, a volar plate, and surrounding tendons. Dorsal dislocations of the PIPJ commonly result from hyperextension injuries and can be classified as Type I-III injuries of increasing severity. Treatment depends on the injury type and stability but generally involves reduction, splinting, and avoiding prolonged immobilization to prevent stiffness. Surgical options may be needed for open injuries or unstable fractures.