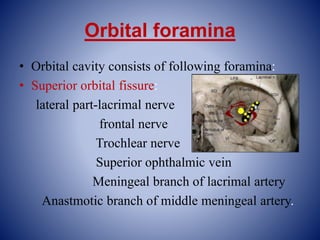
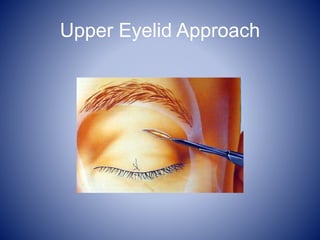
This document provides an overview of the anatomy of the orbit, including its osteology, contents, innervation, vascular supply, and implications in maxillofacial injuries. Key points discussed include the bones that form the orbital walls, contents such as the eyeball and extraocular muscles, nerves like the oculomotor and branches of the trigeminal, and arterial supply from the ophthalmic artery. Maxillofacial fracture patterns involving the orbit like Lefort II and III are described.