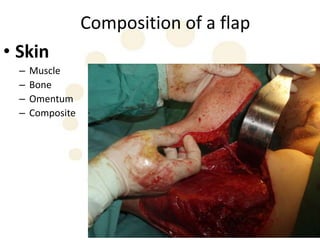
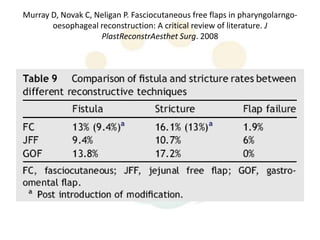
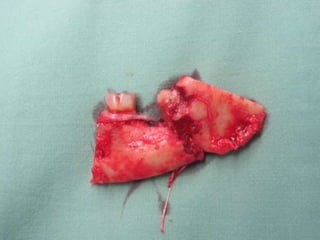
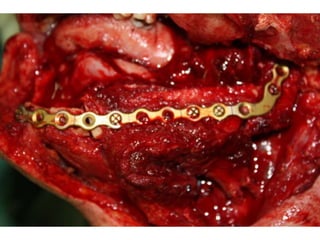
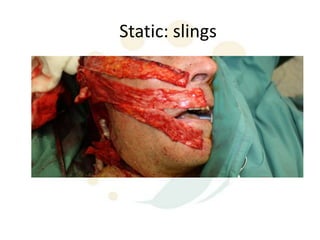
Flaps and grafts are used in reconstructive surgery to restore form and function. A flap maintains its blood supply, and can be skin, muscle, bone or composite tissue transferred from a donor site. Key differences between flaps and grafts are discussed. Various flap types - local, regional, free etc. - are characterized by their components and blood supply. Reconstructive goals include separating cavities, restoring function and swallowing. Literature on fistula and stricture rates after pharyngeal reconstruction with different flaps is reviewed. Mandible and tongue reconstruction examples using flaps are provided.