




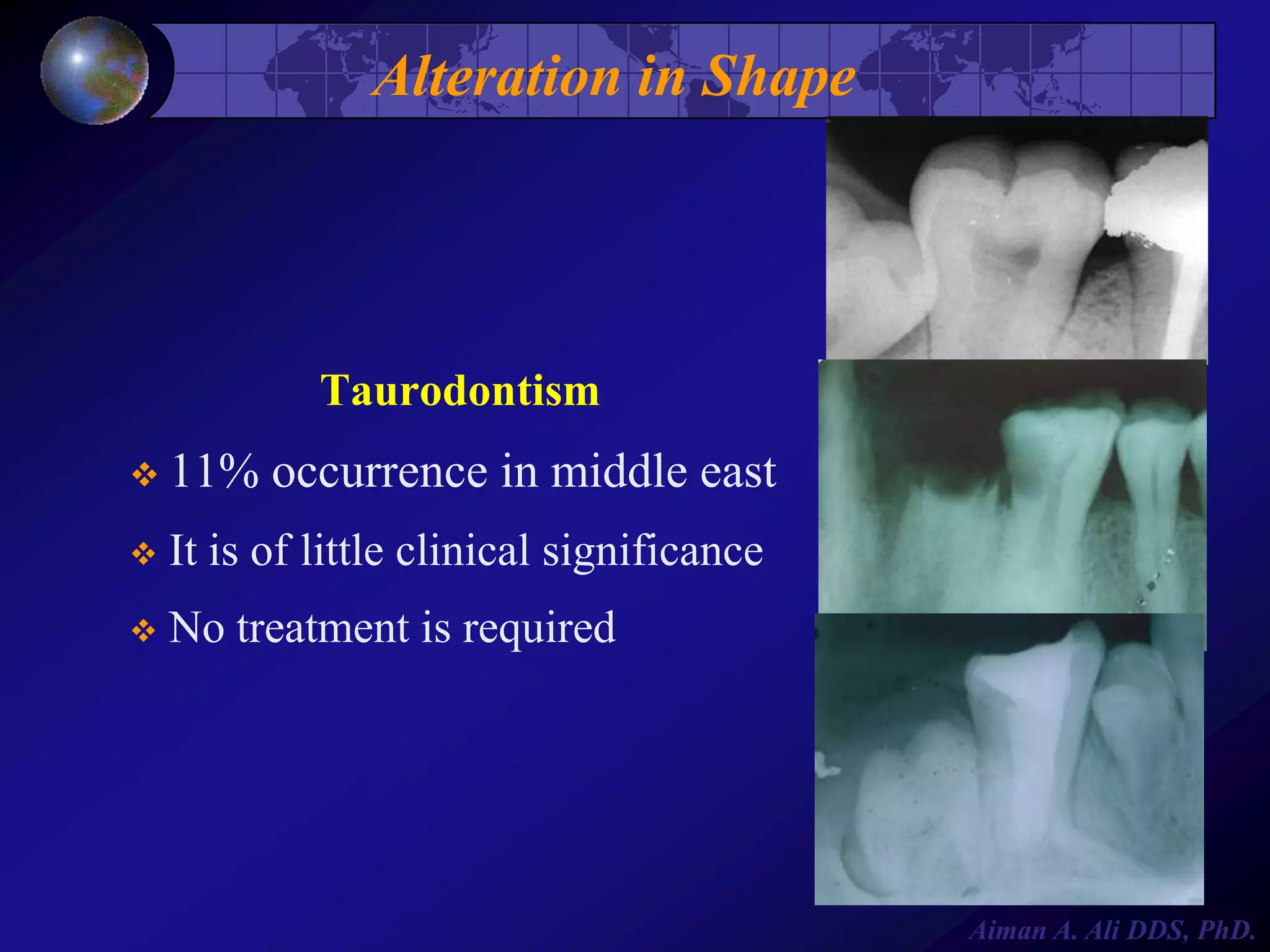

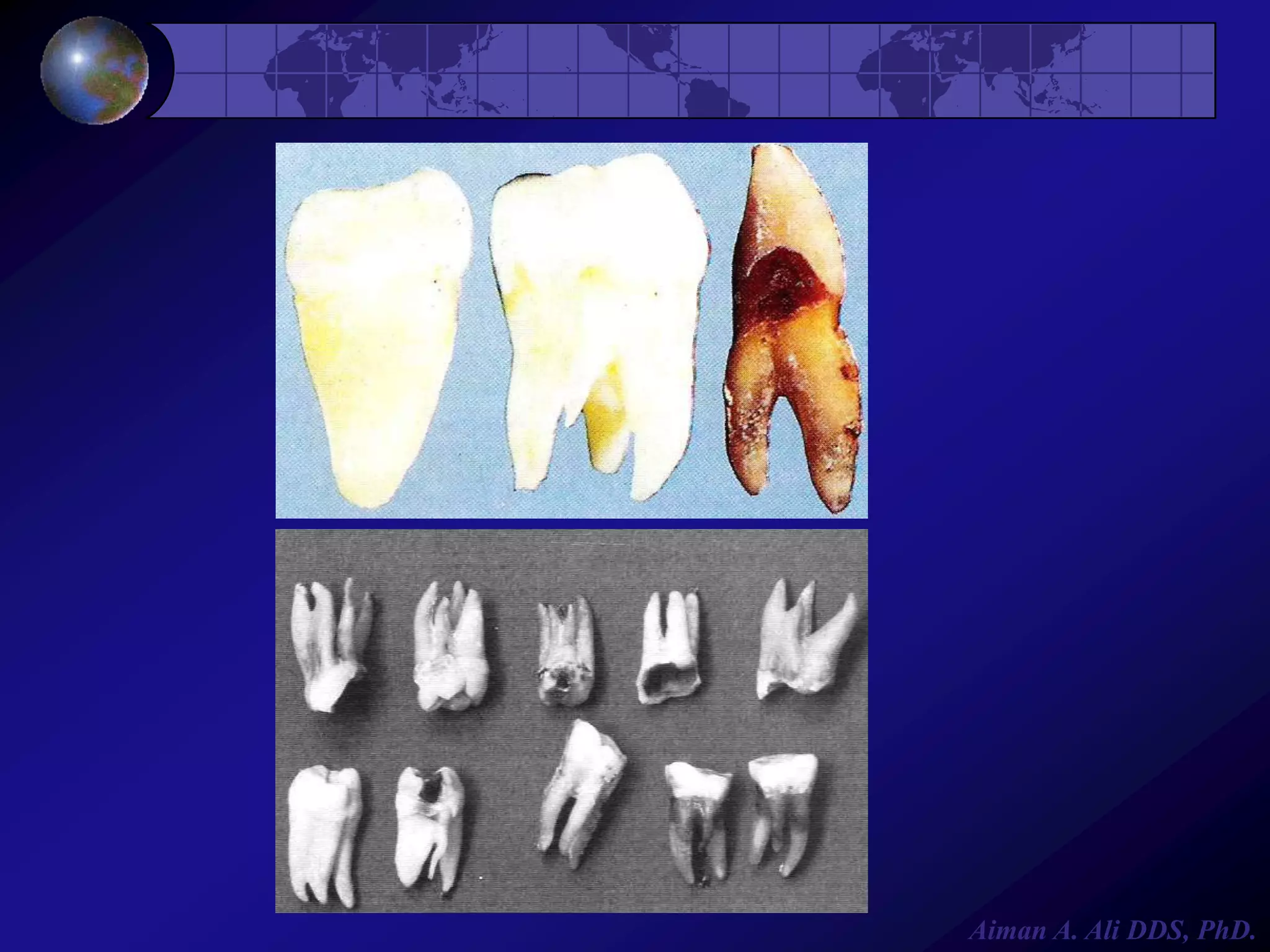
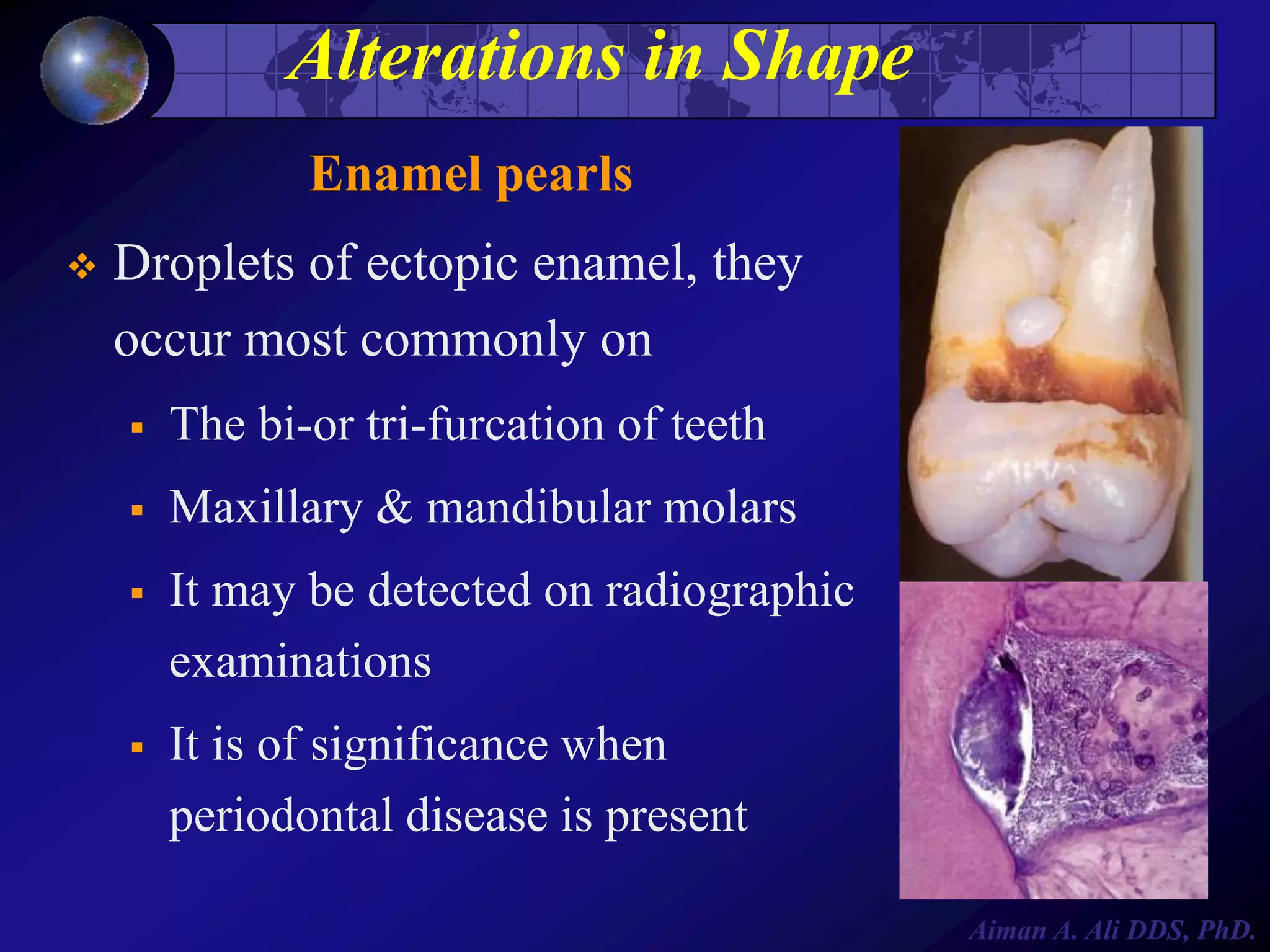
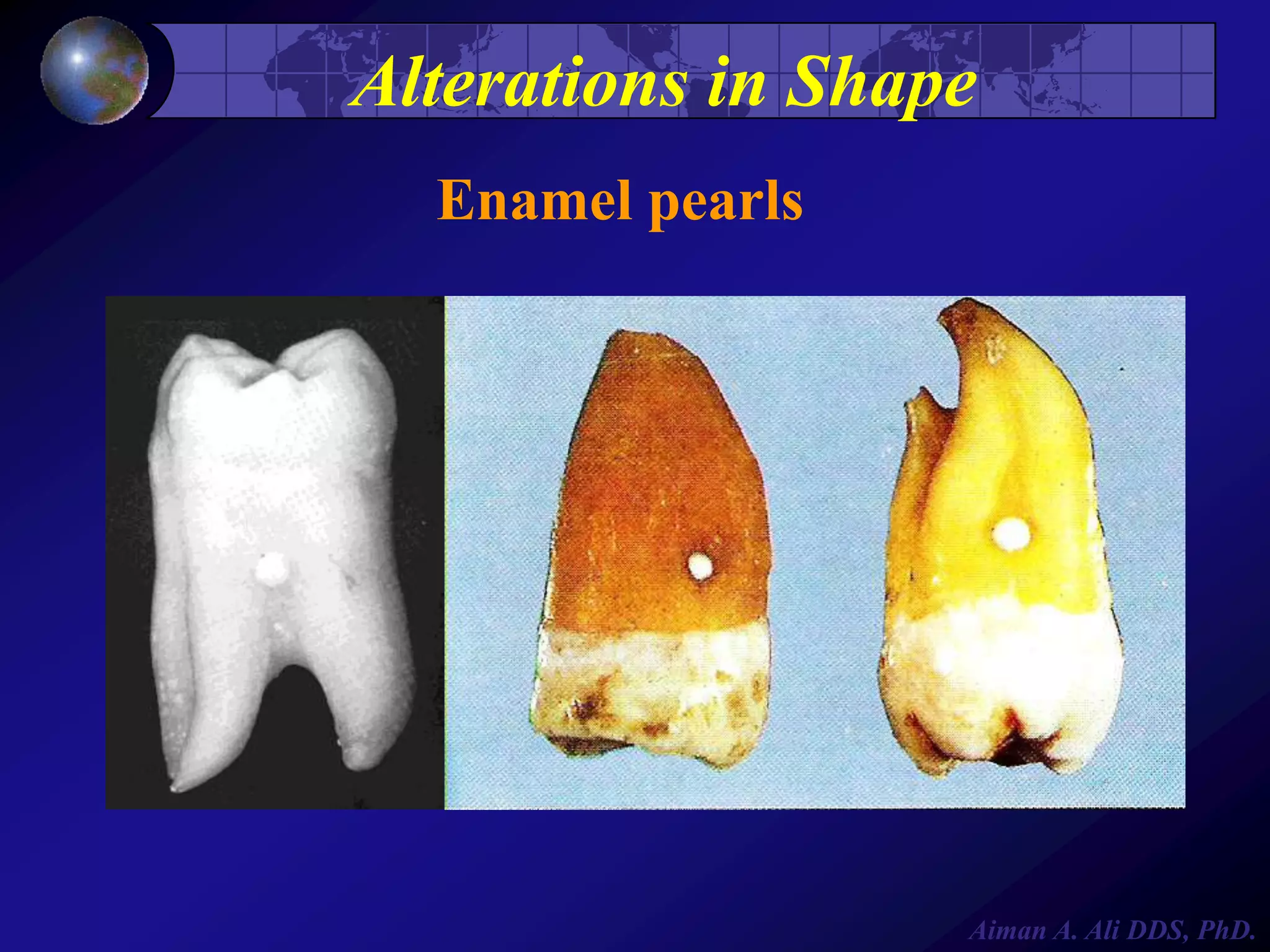
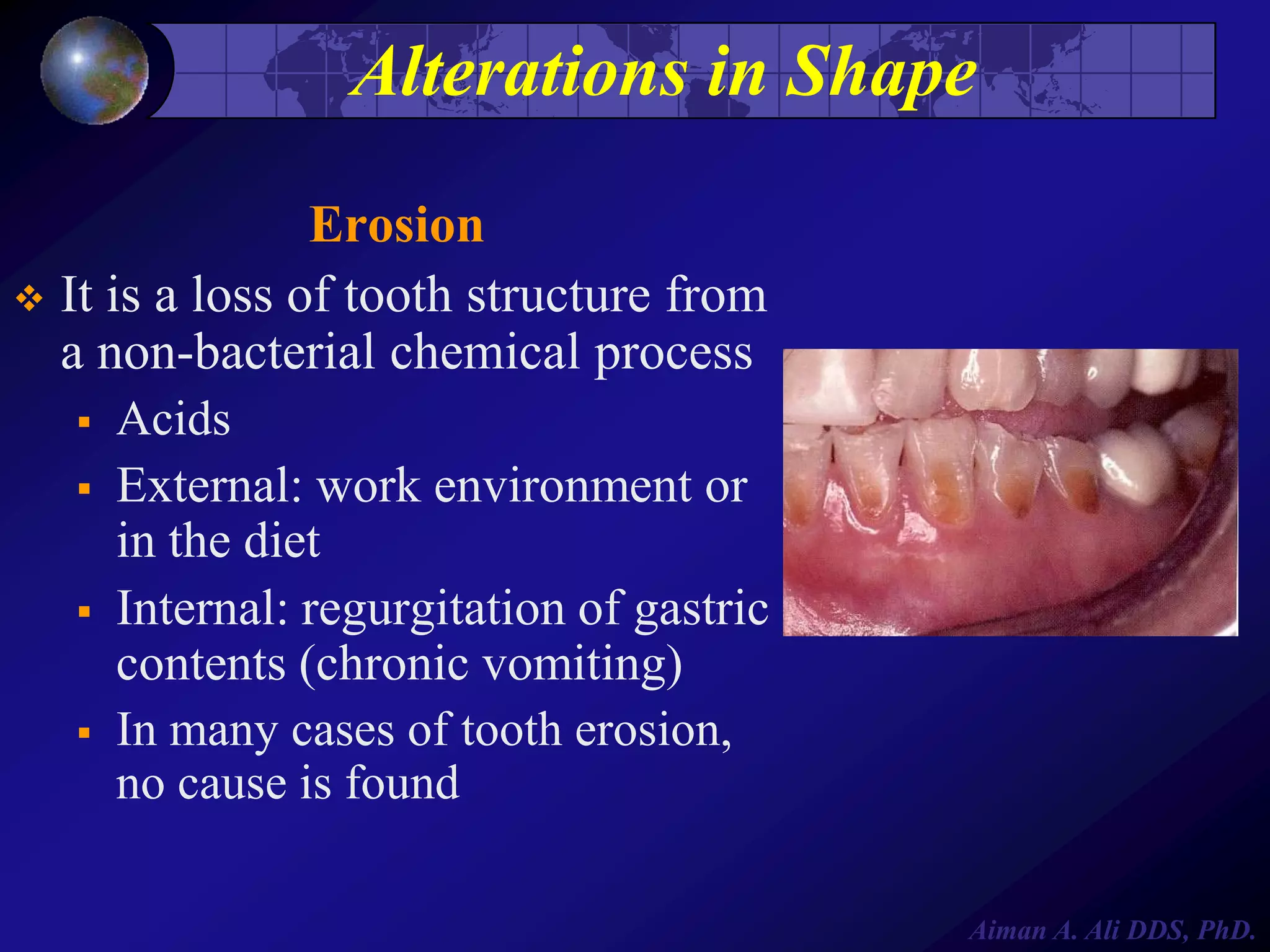
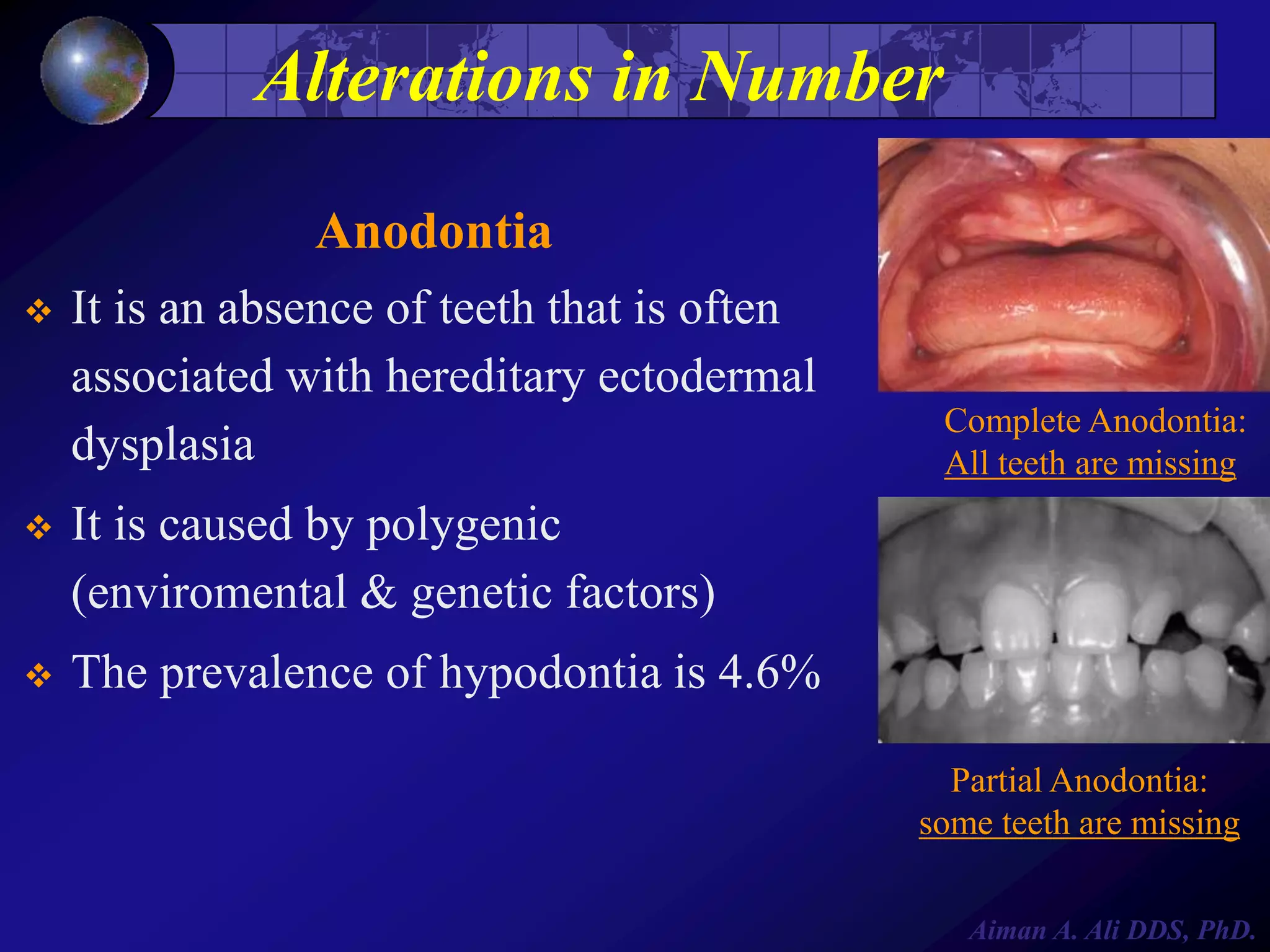

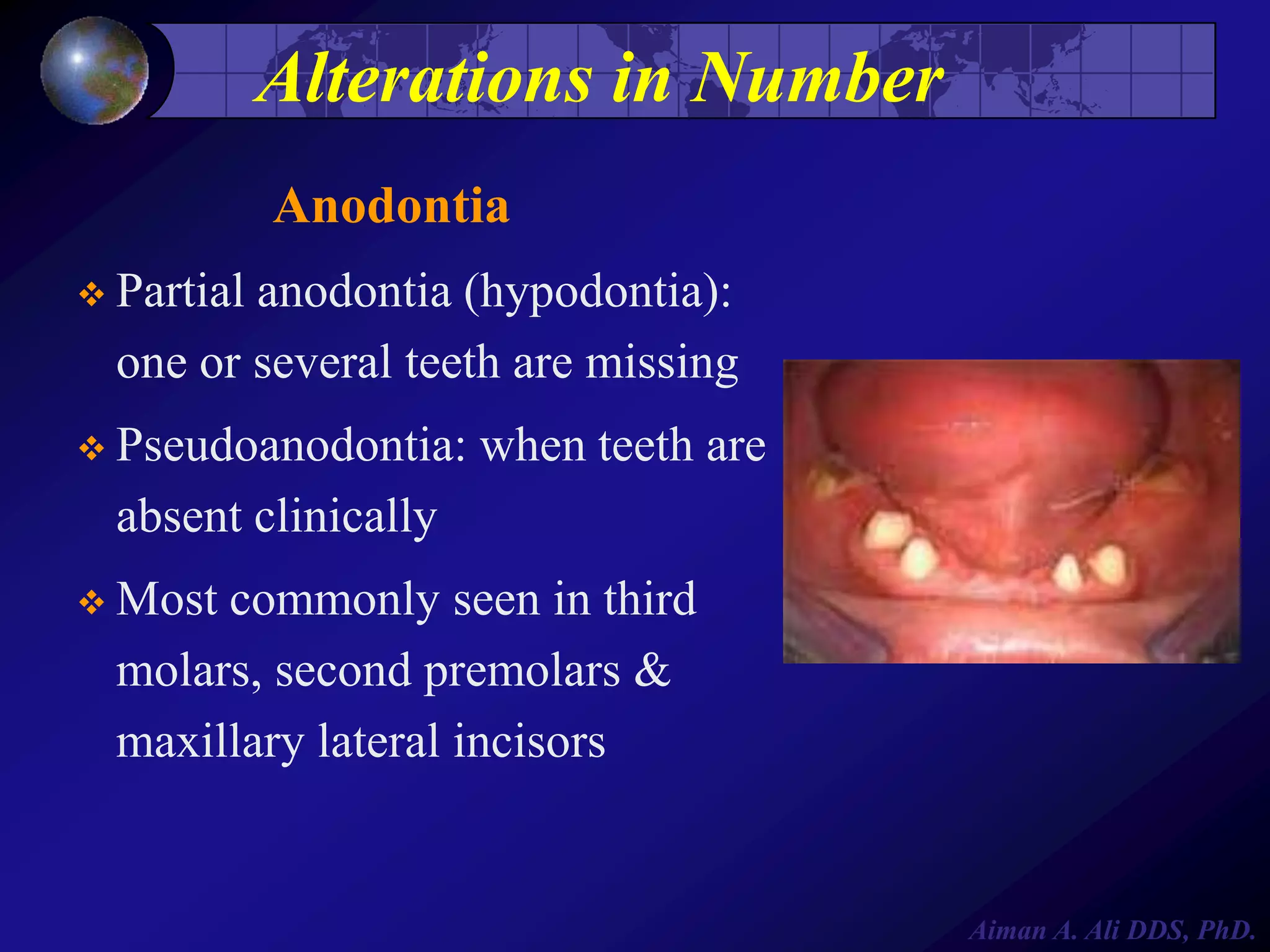


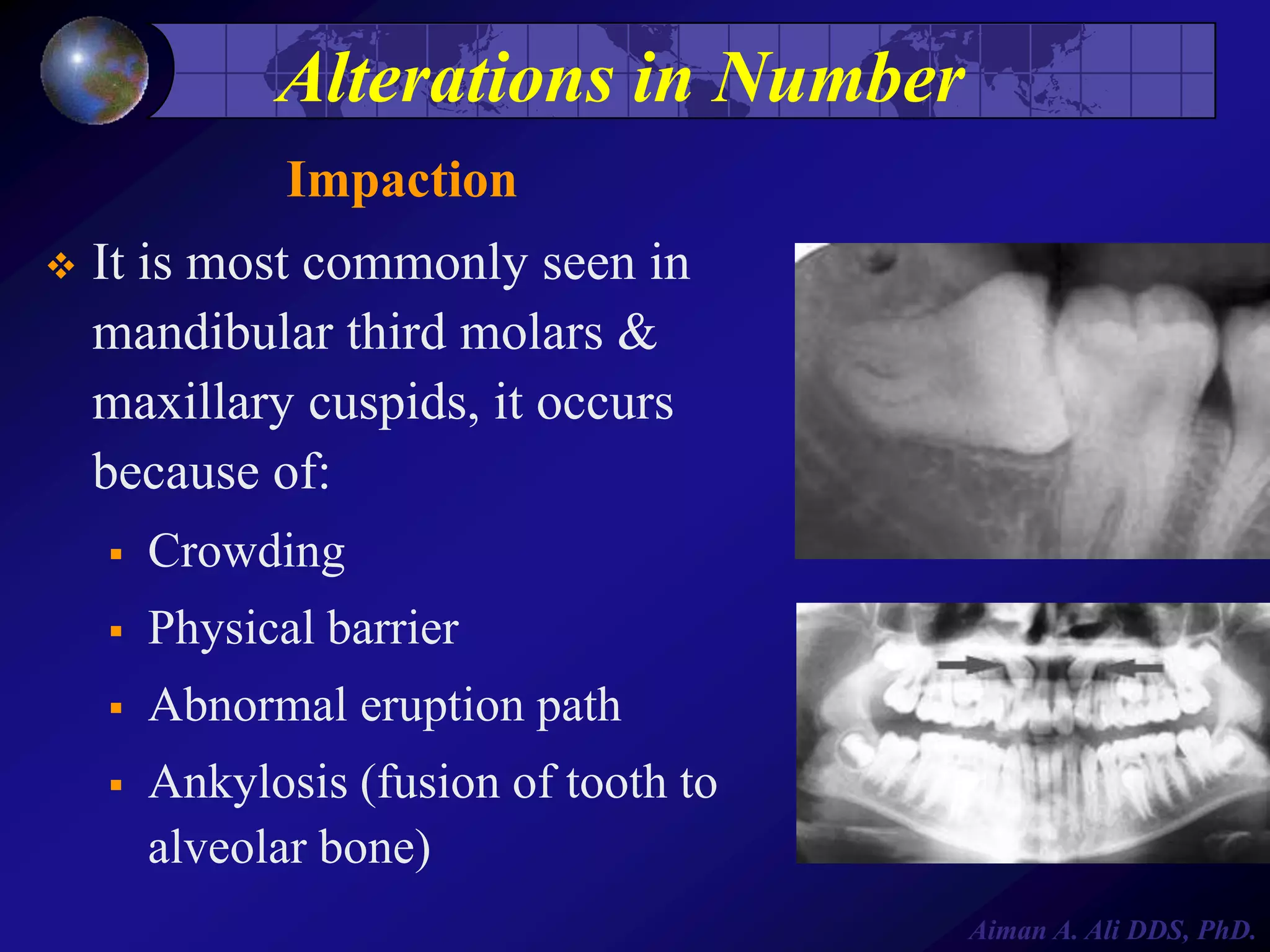
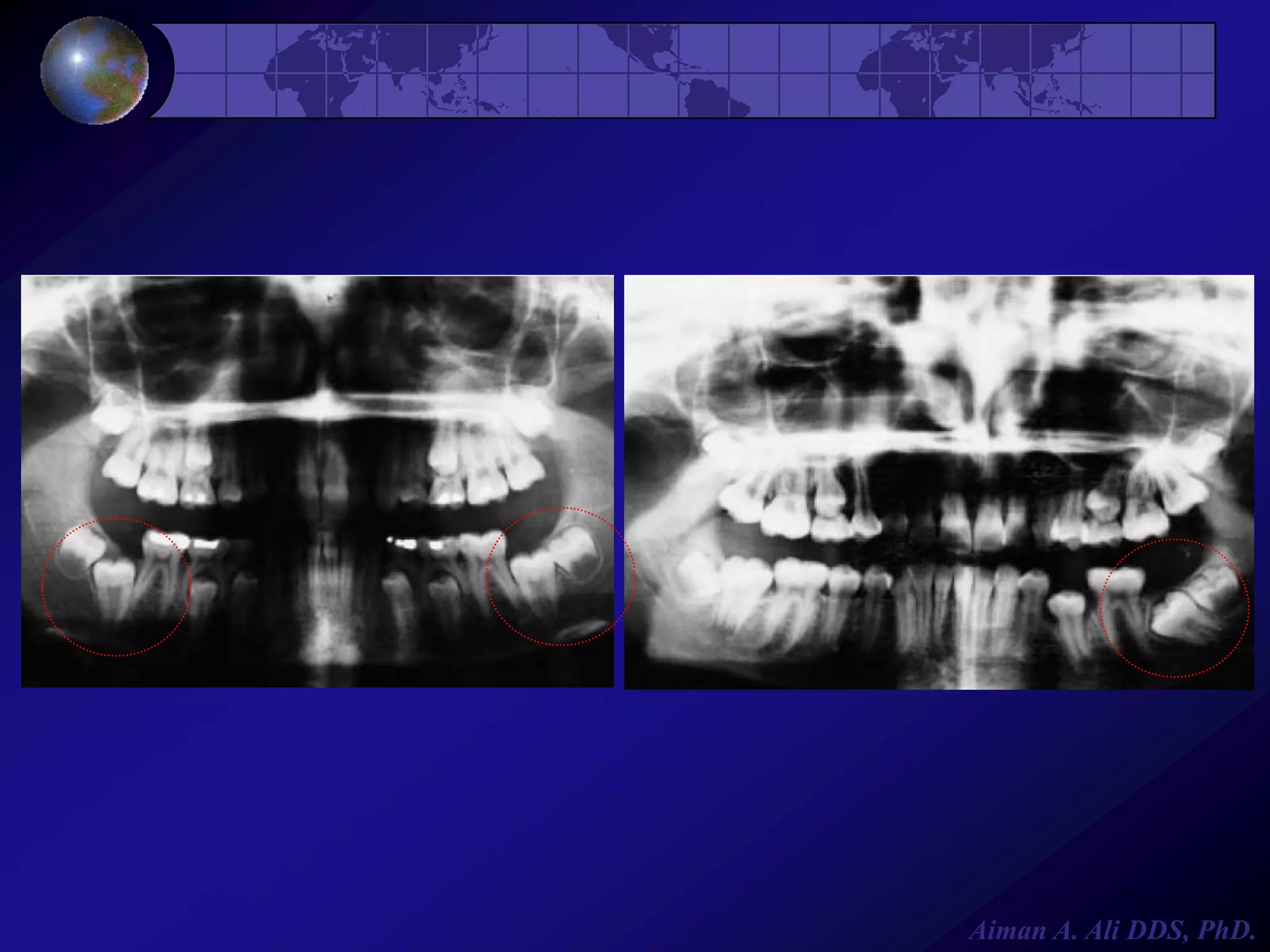
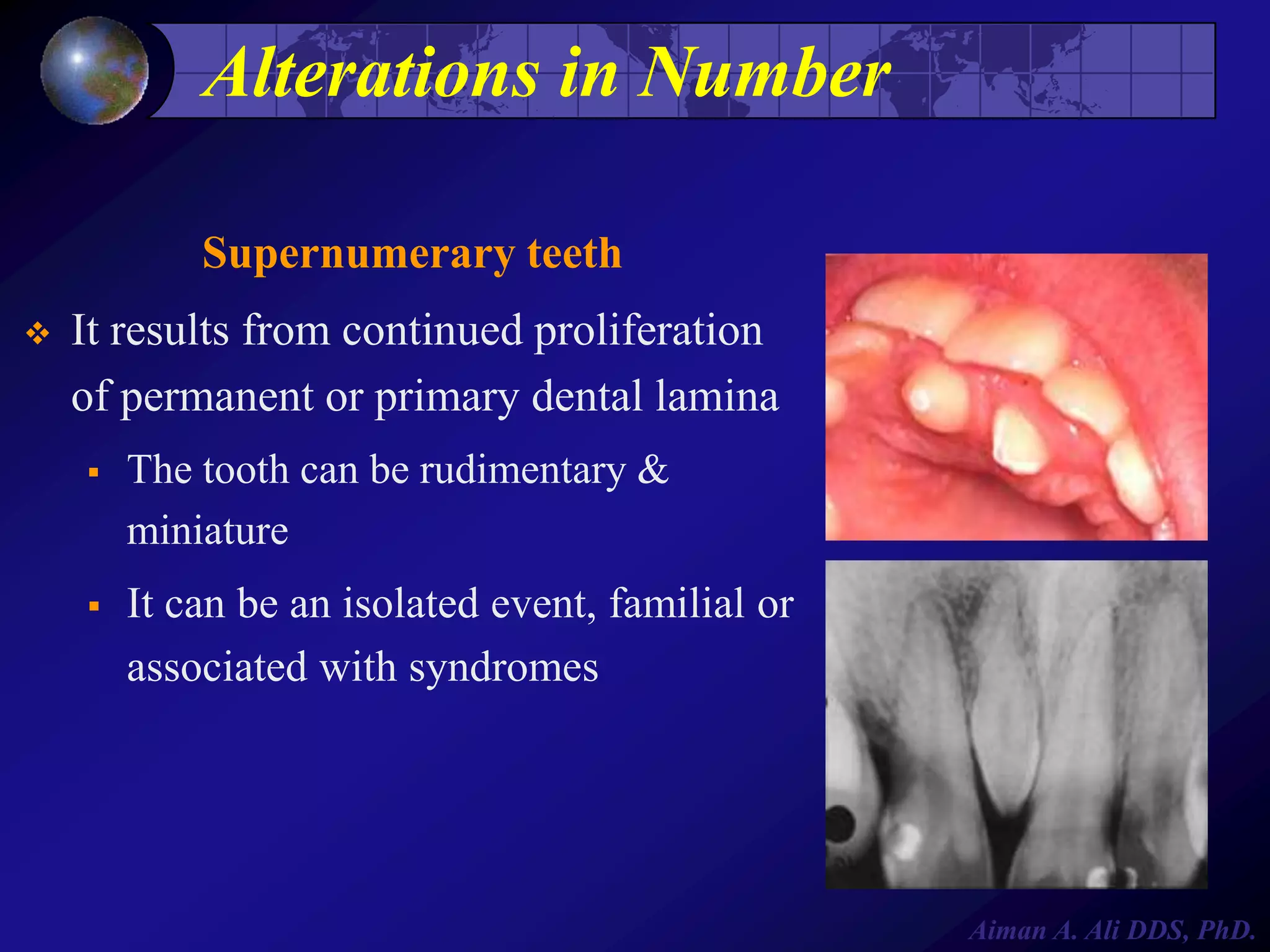
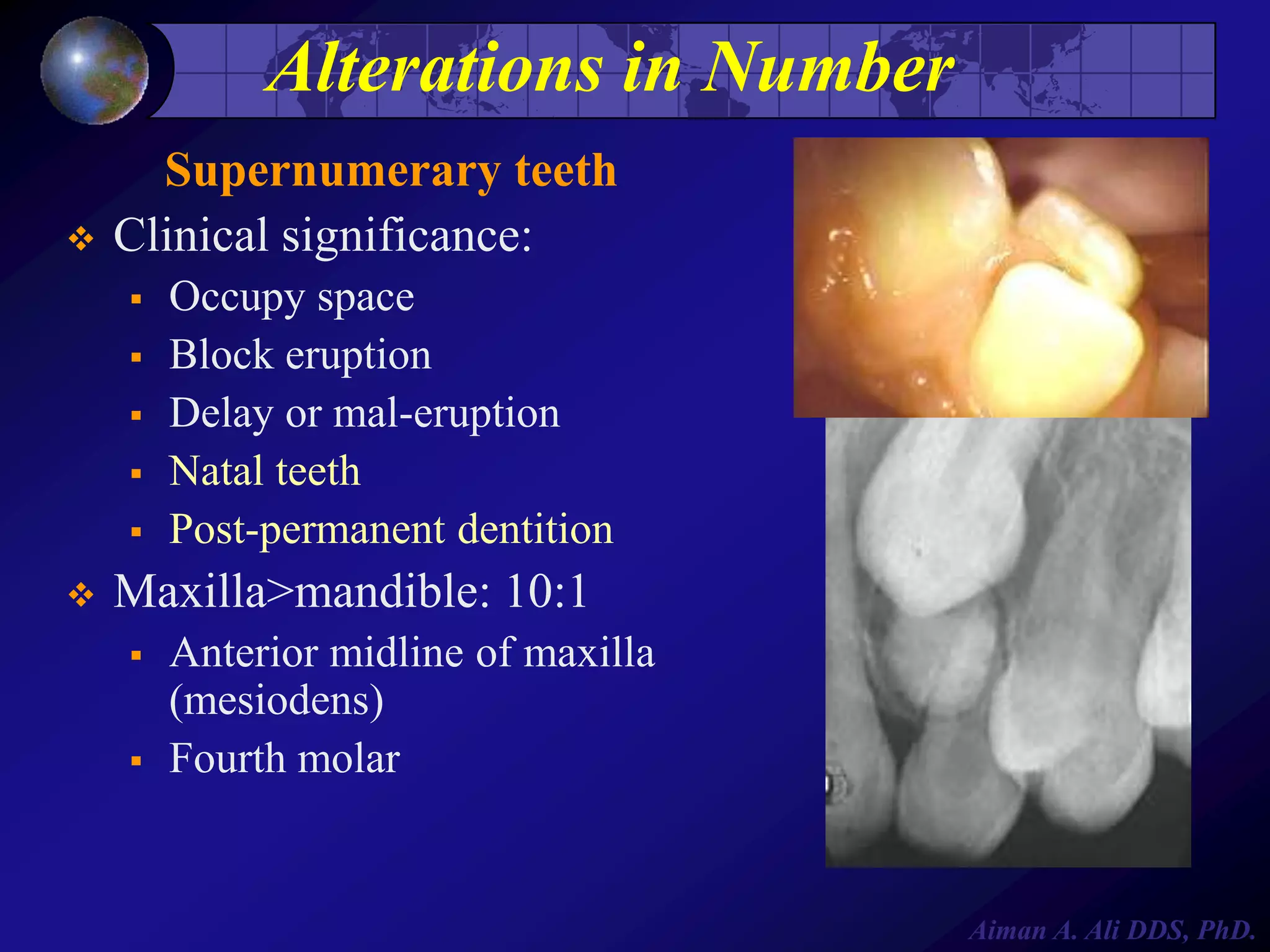
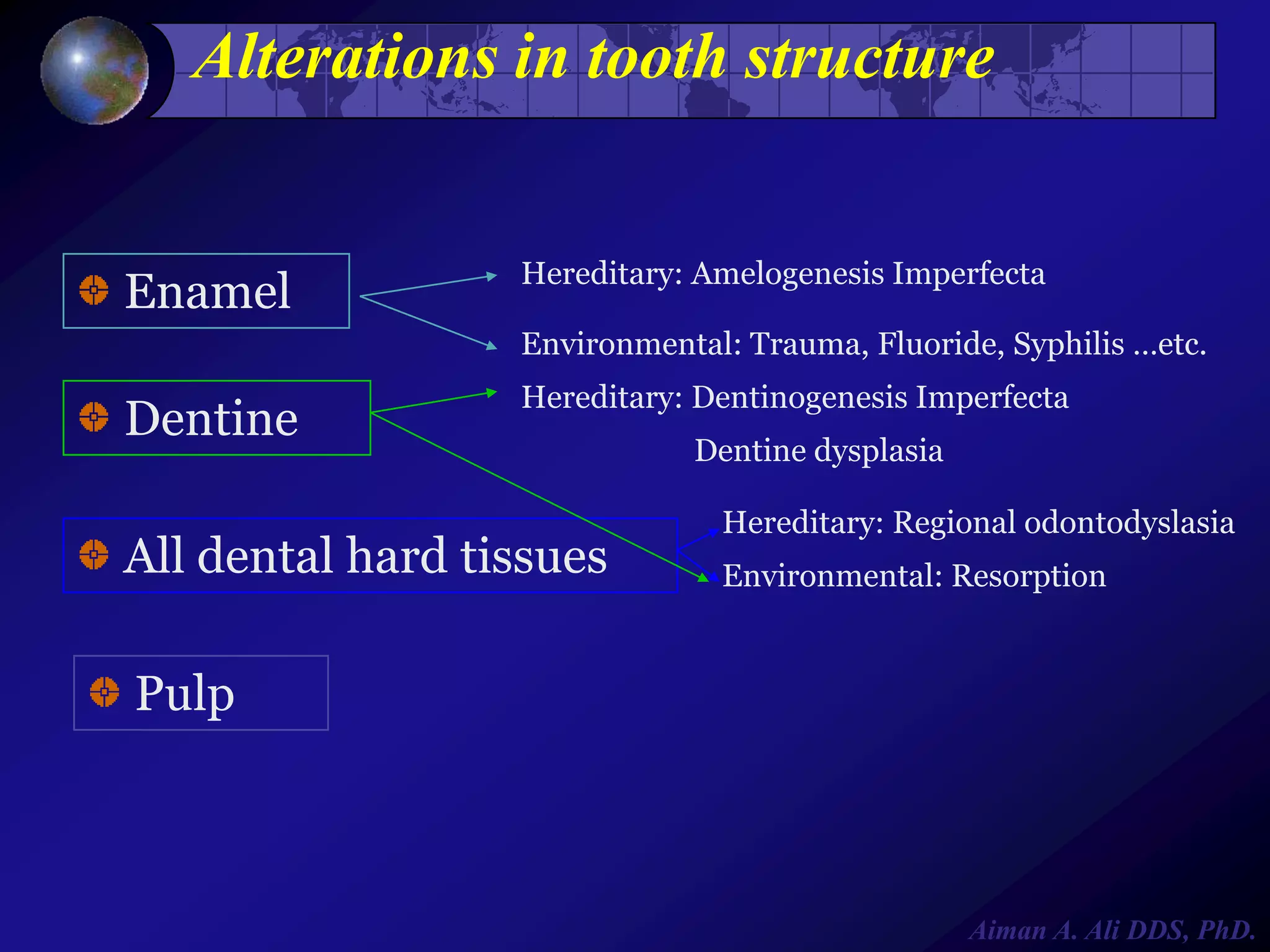




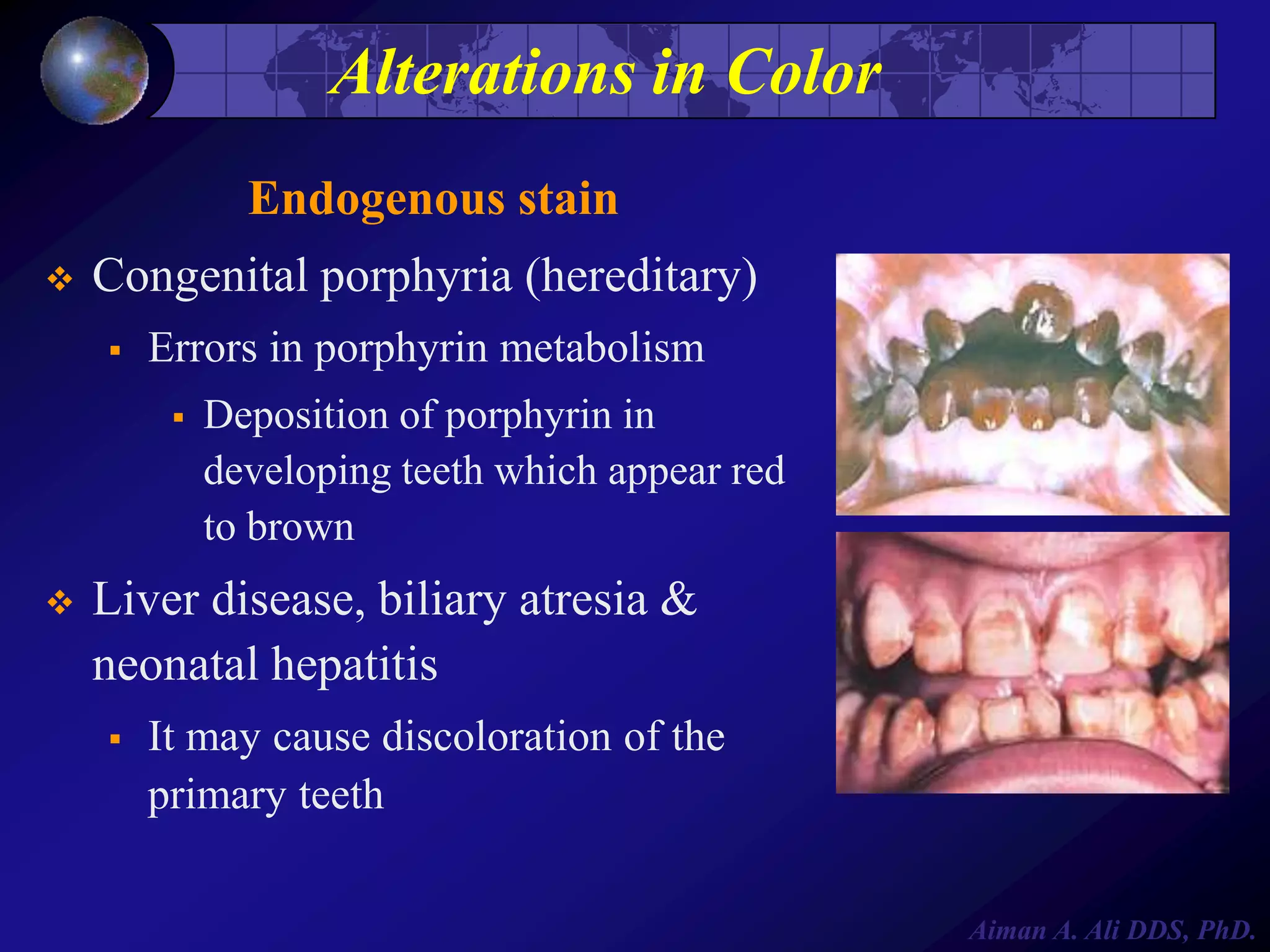
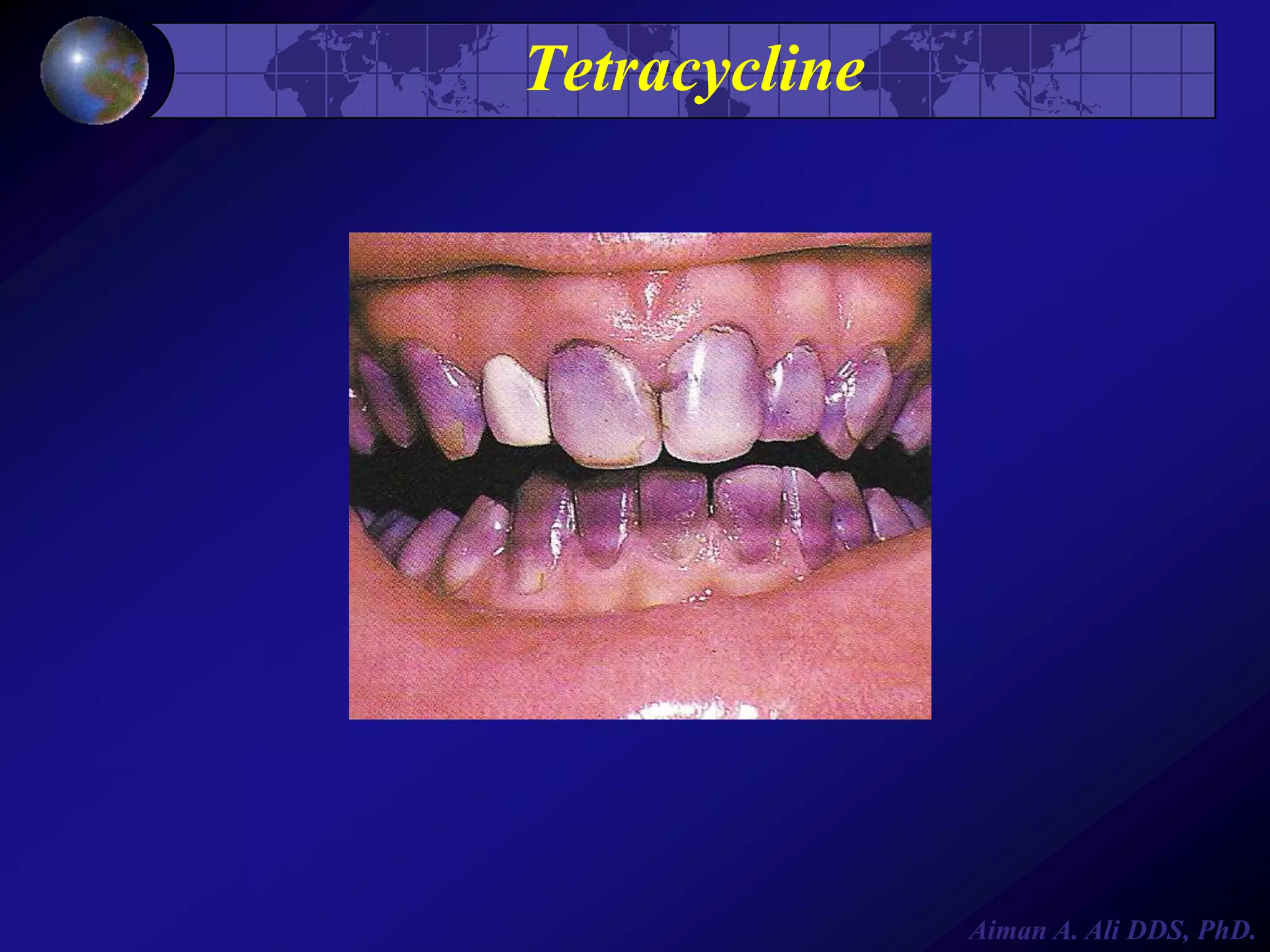



This document outlines the course content for Oral Pathology I taught by Dr. Aiman A. Ali. The course covers abnormalities of teeth and oral tissues including alterations in size, shape, number, structure and color of teeth. Specific conditions discussed include microdontia, taurodontism, gemination, fusion, impaction, and amelogenesis imperfecta. Evaluation includes attendance, quizzes, exams and case presentations. The document provides the syllabus, lecture topics, and expectations for the laboratory component where students will examine abnormalities of teeth and oral tissues.































































































