Downloaded 762 times




















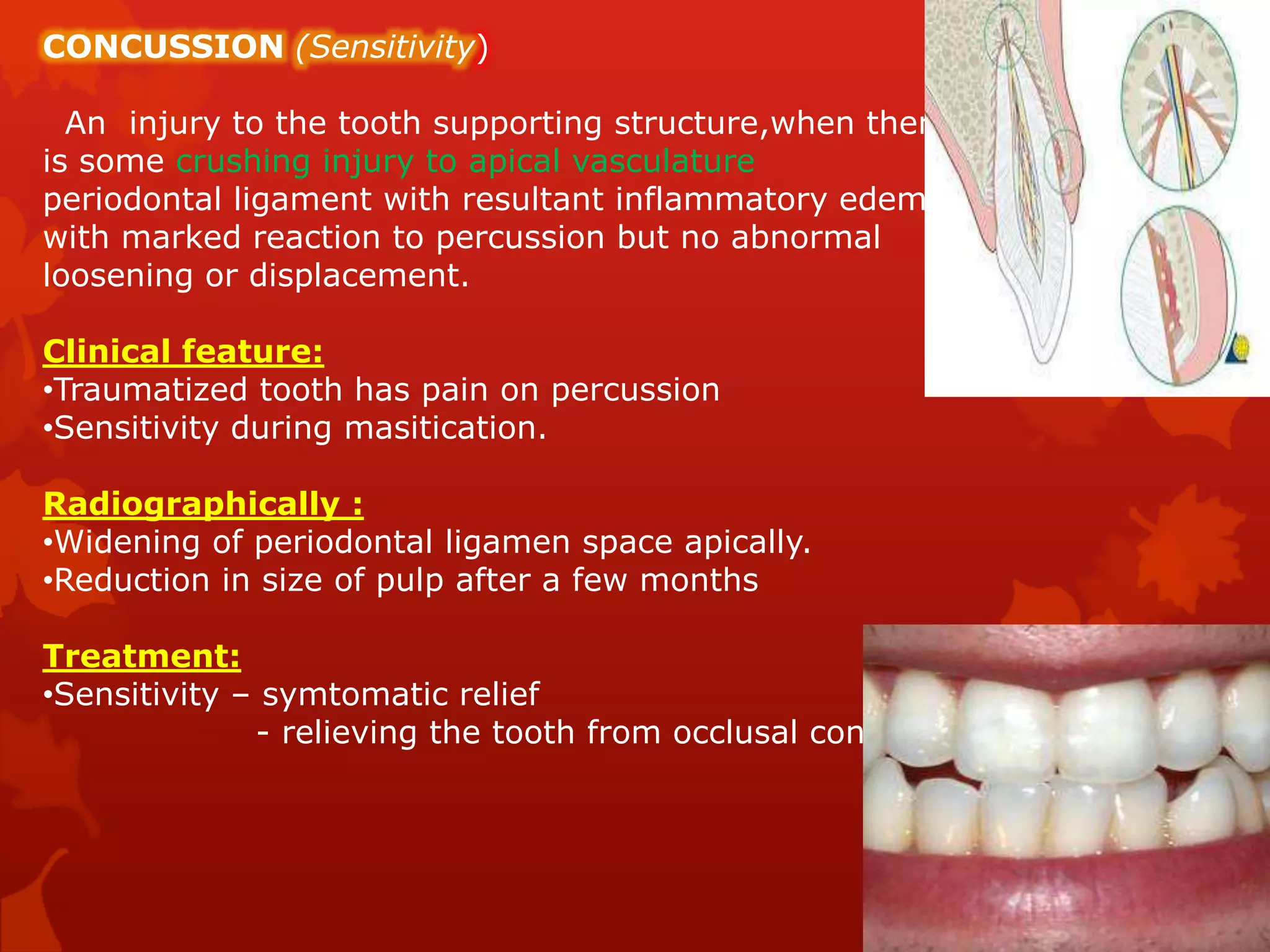















The document summarizes traumatic dental injuries and their management. It discusses the classification, clinical features, treatment, and stabilization periods for various types of dentoalveolar injuries including enamel fractures, crown fractures, root fractures, luxations, and avulsions. Splinting is described as the best method for immobilizing mobile teeth or displaced teeth, with different splinting techniques and materials discussed. Prompt treatment of dental trauma is emphasized to save injured teeth.























































































