Downloaded 476 times
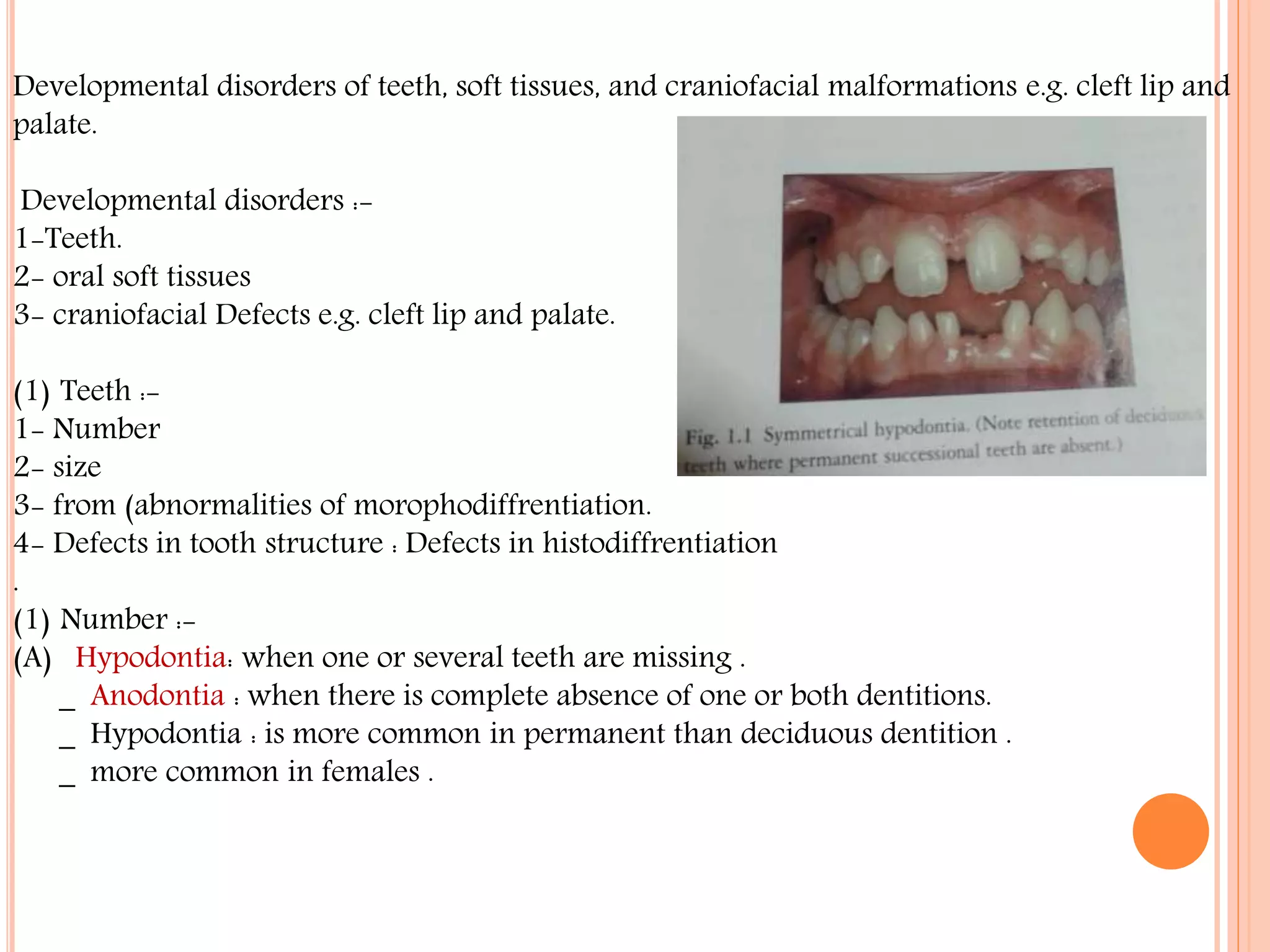
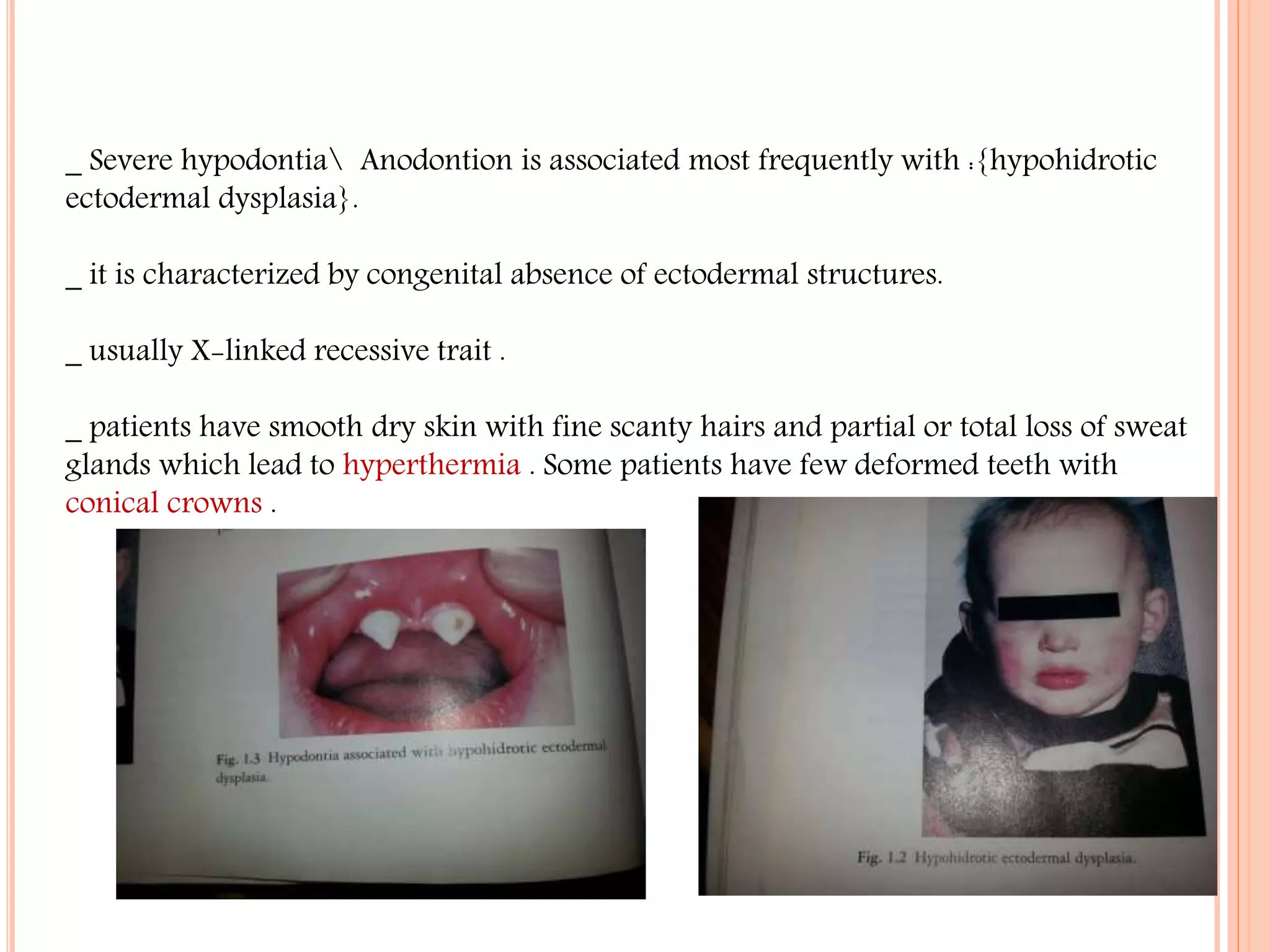


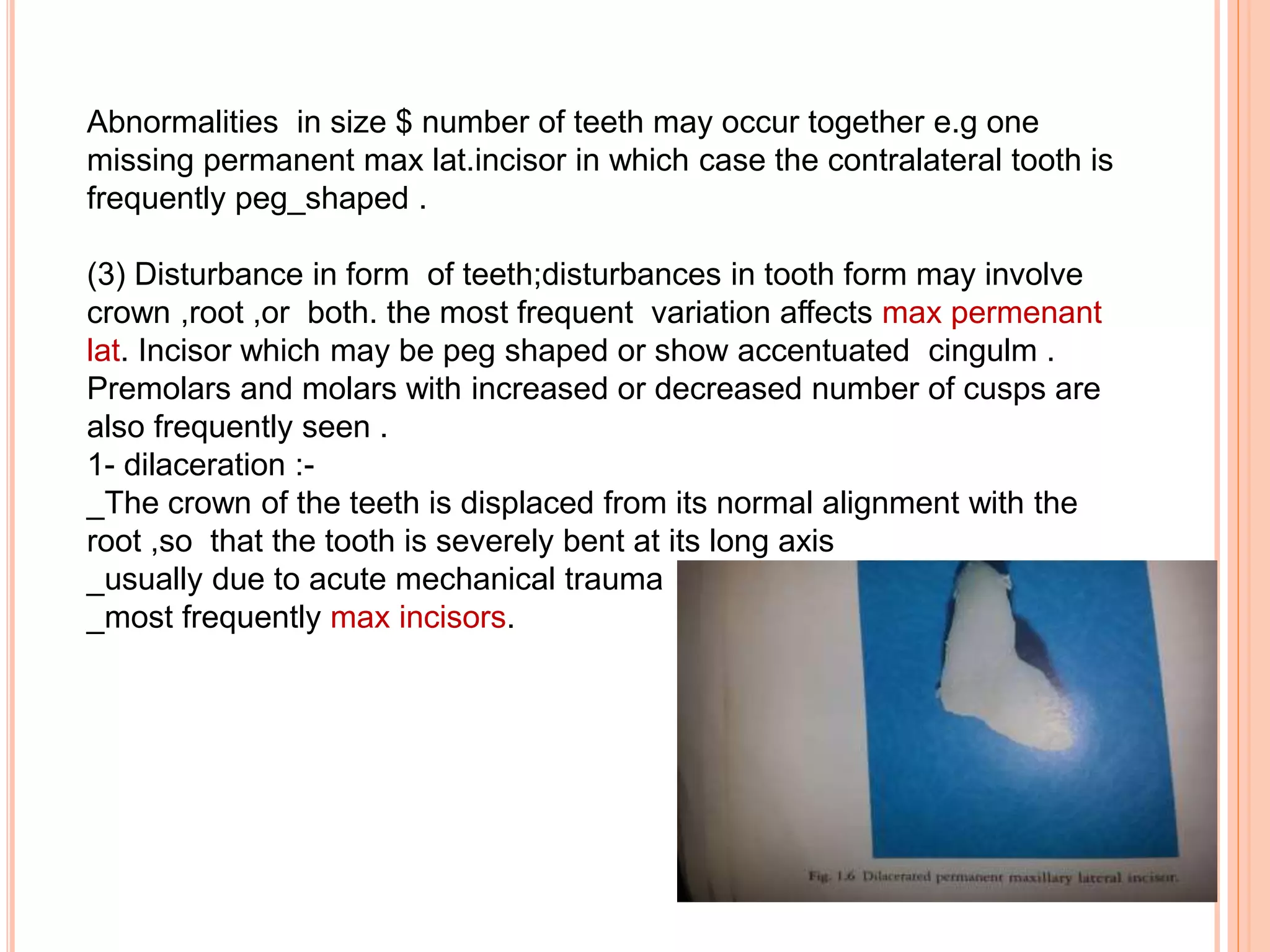















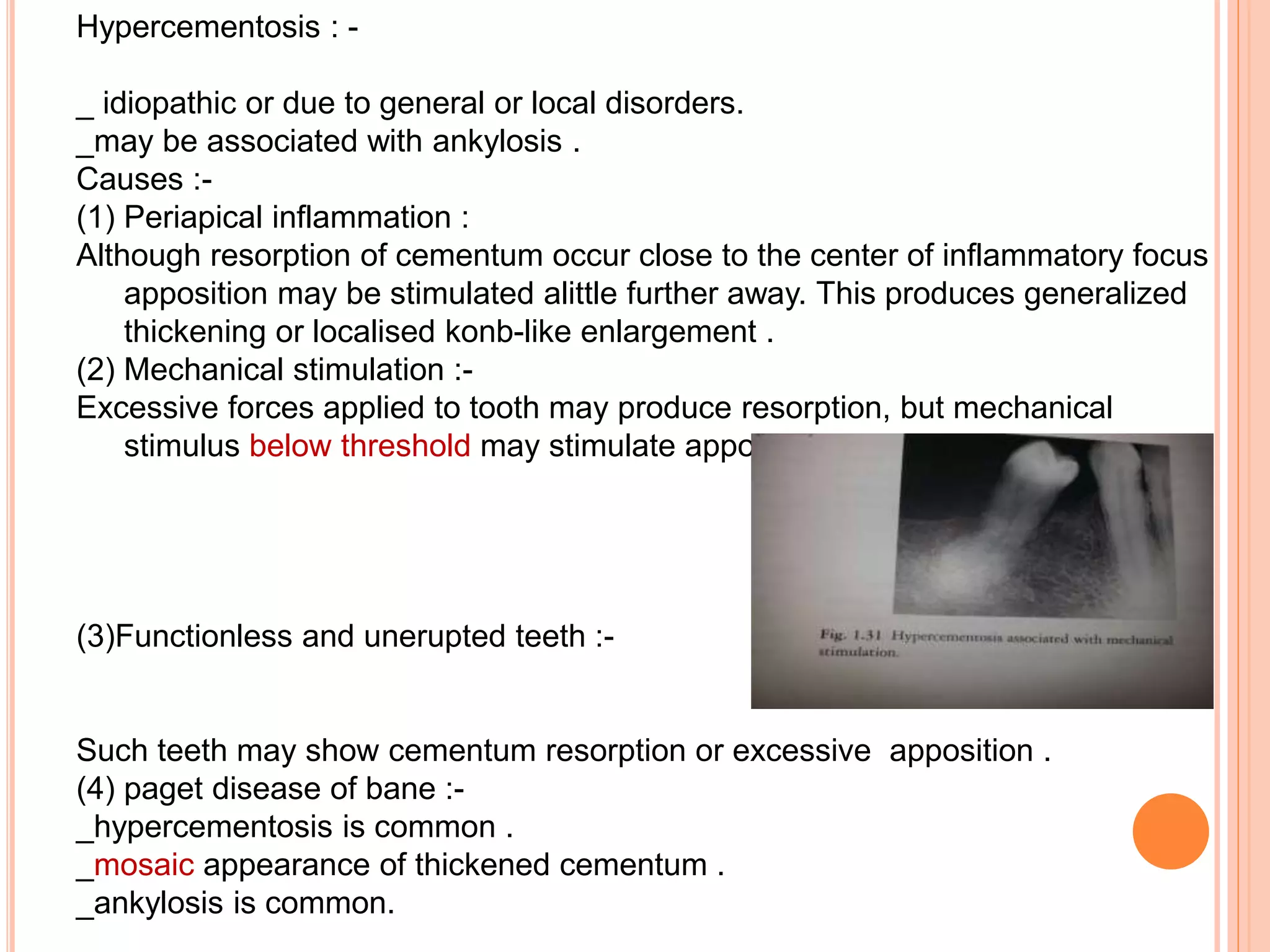















This document discusses developmental disorders of teeth, soft tissues, and craniofacial structures. It focuses on abnormalities in teeth, including number (hypodontia, hyperdontia), size (macrodontia, microdontia), form (shape abnormalities, taurodontism, double teeth), and structure (enamel hypoplasia, hypomineralization, dentin abnormalities). Causes may be local such as infection or trauma, or systemic like genetic conditions, environmental factors during tooth development, or nutritional deficiencies.























































































