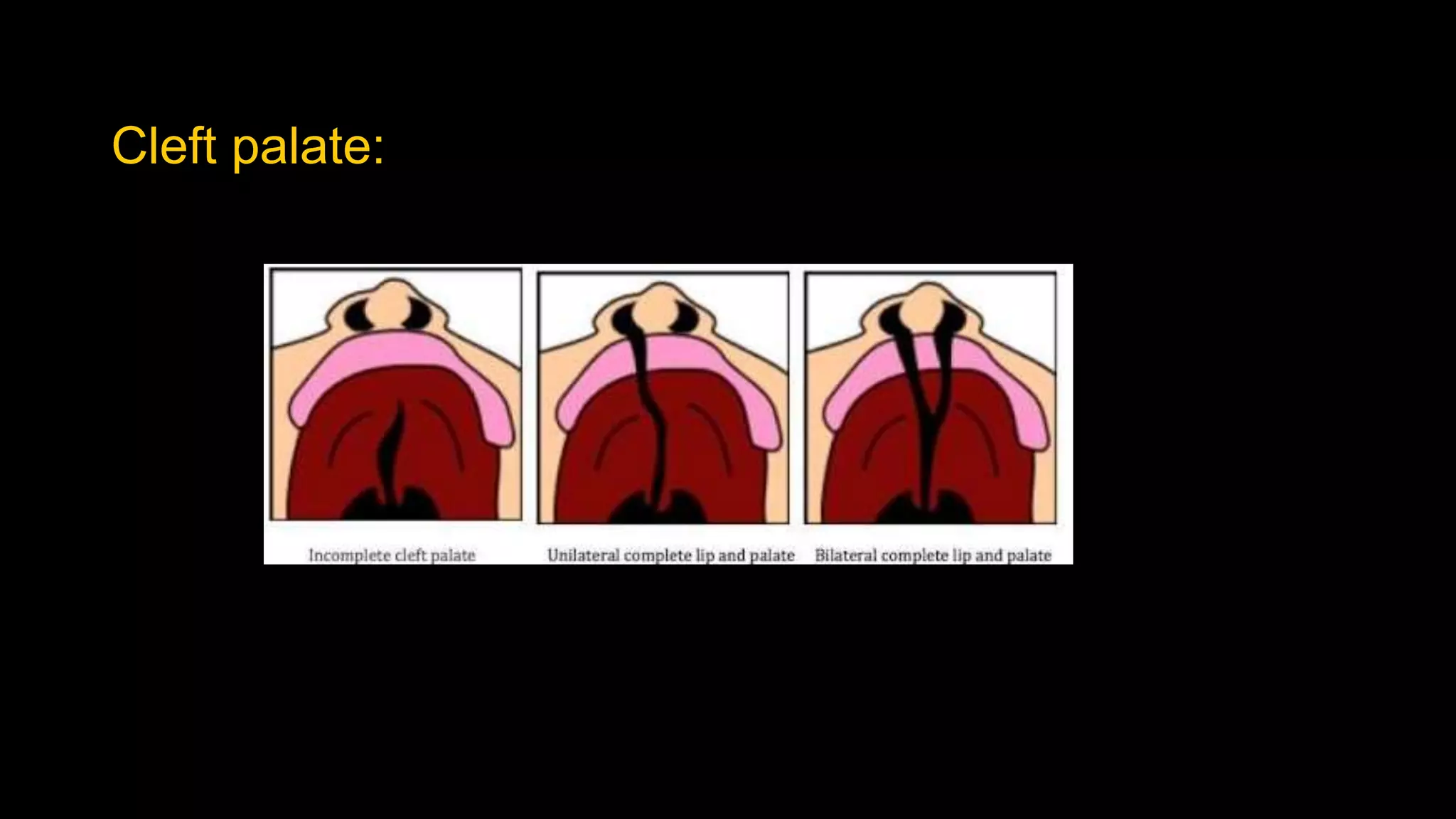
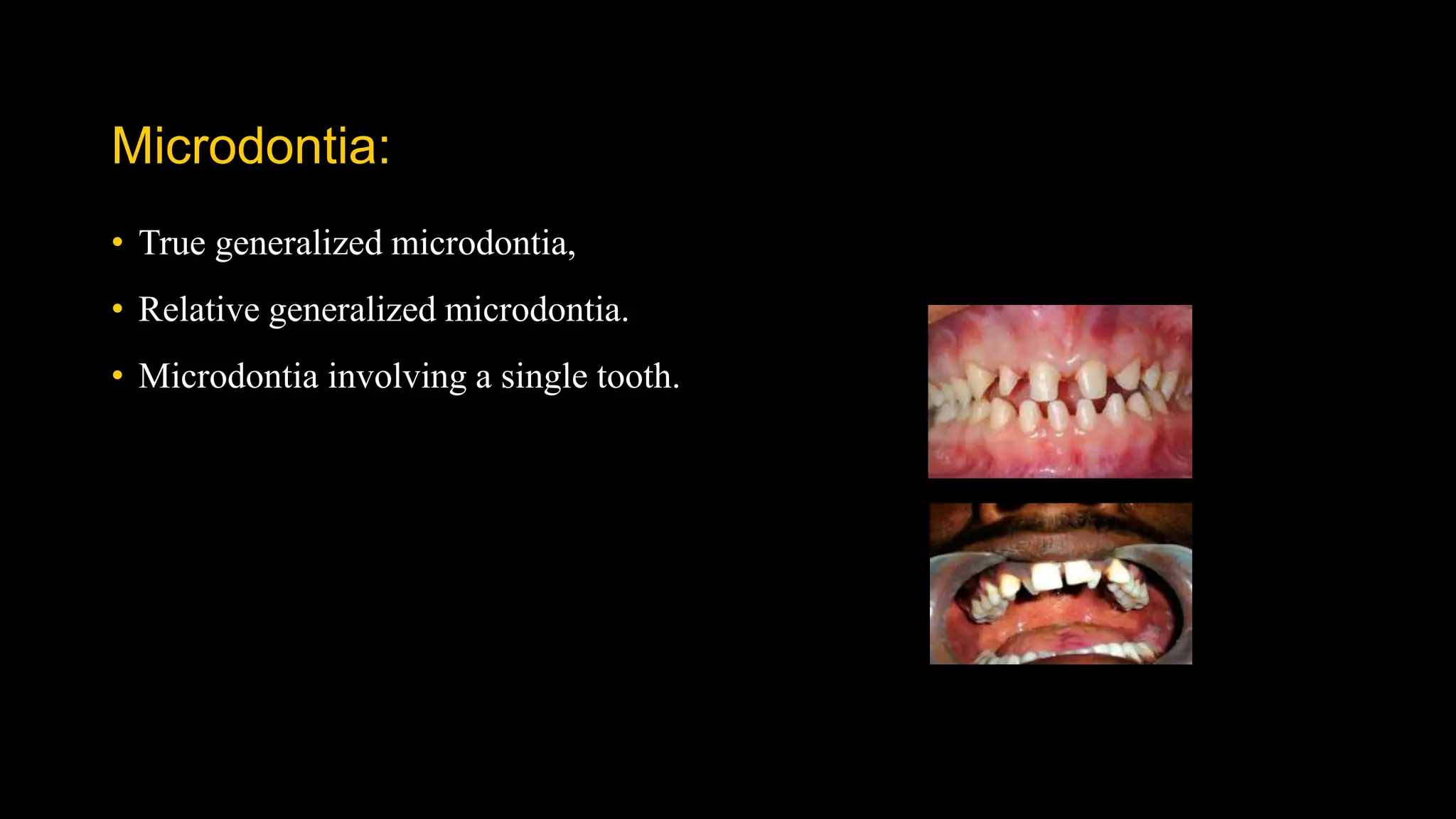
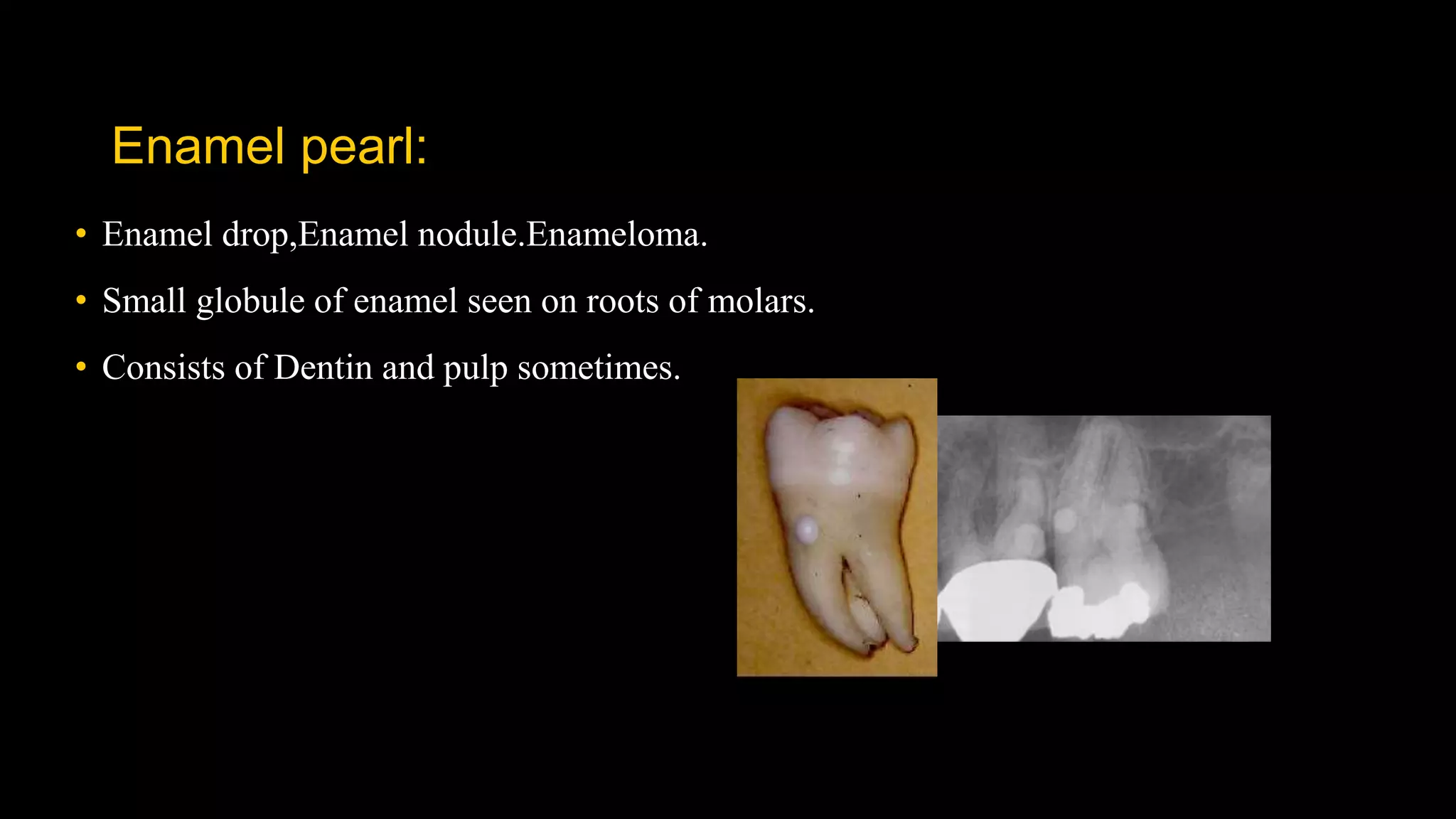
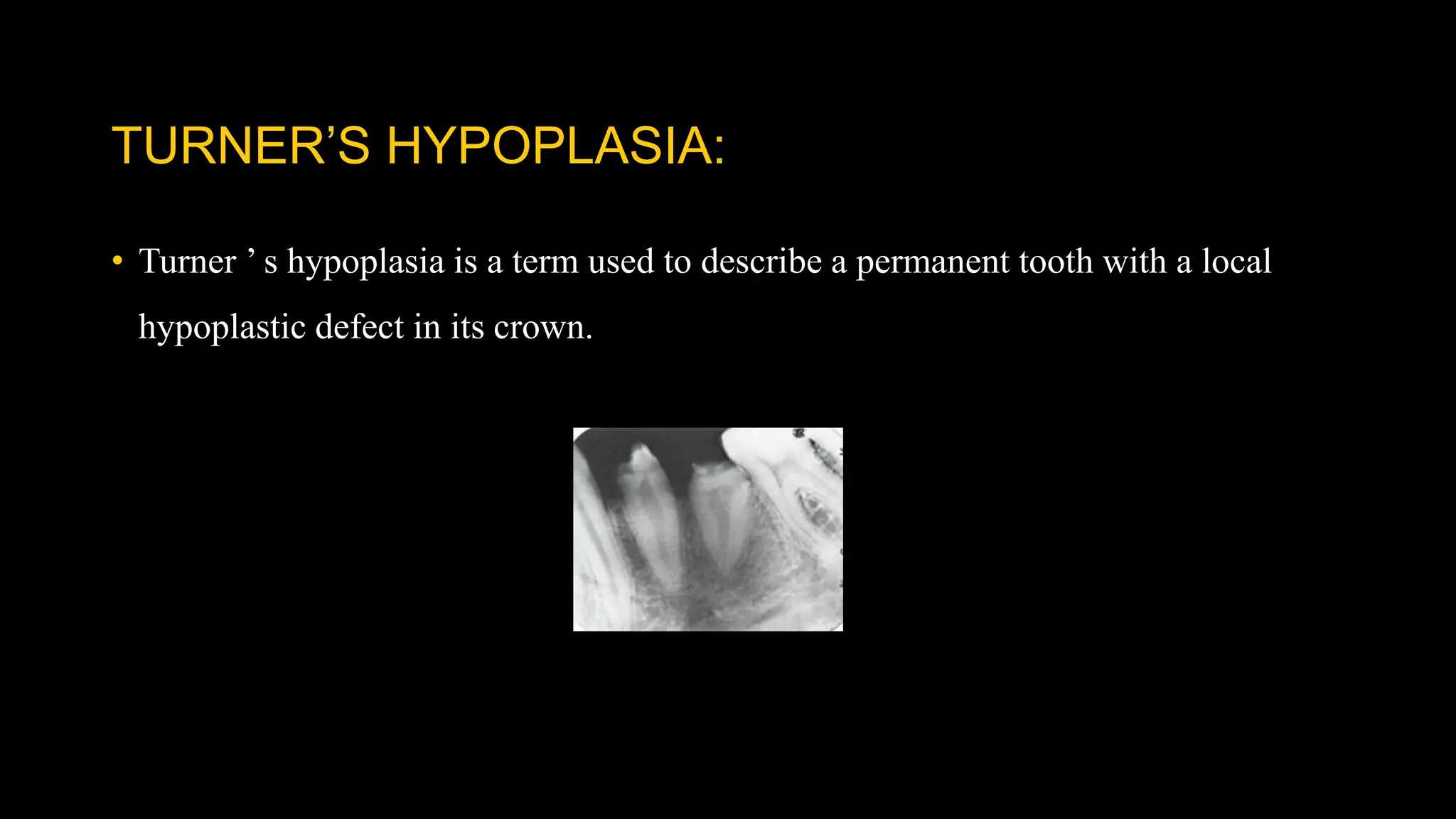
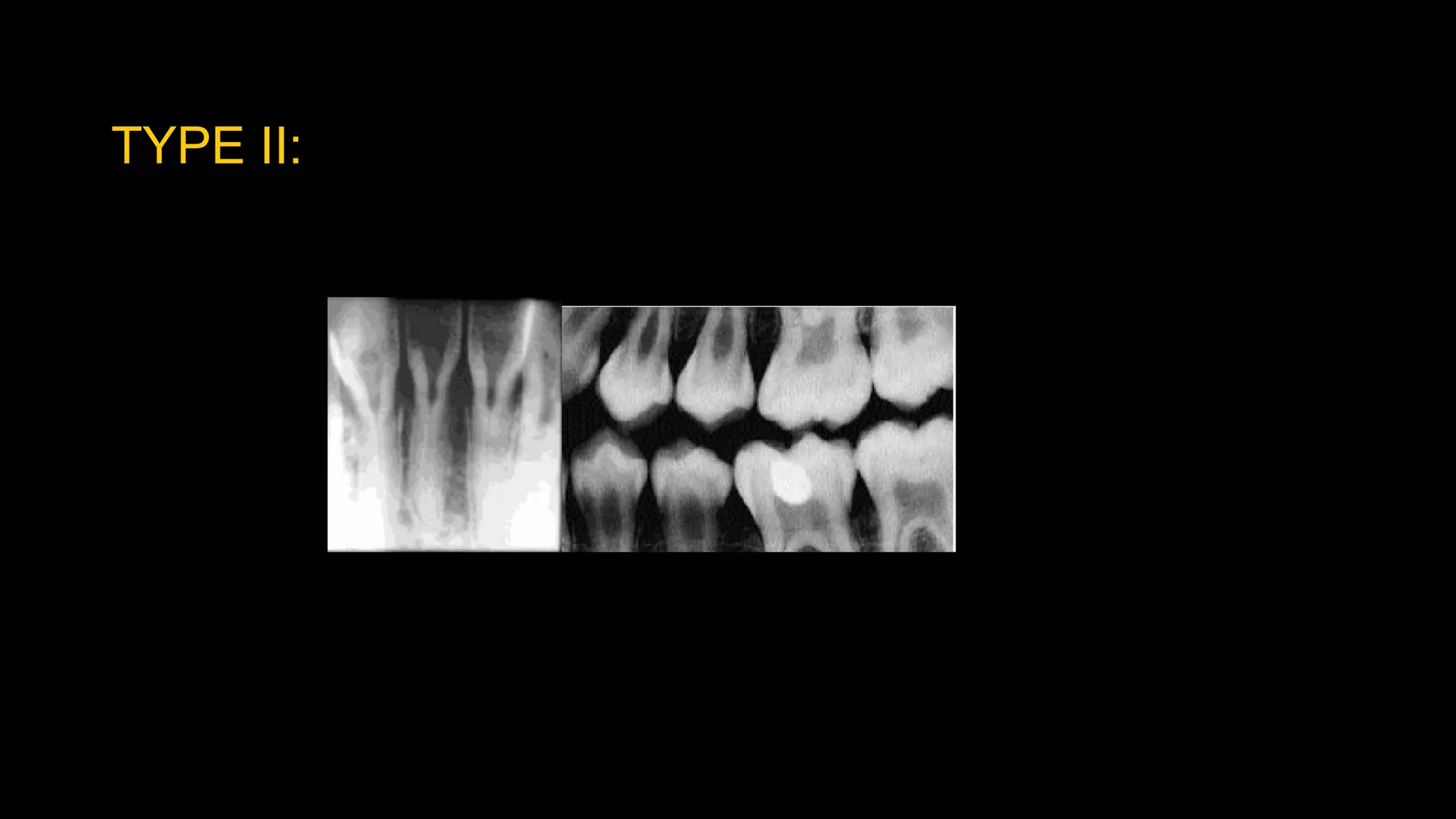
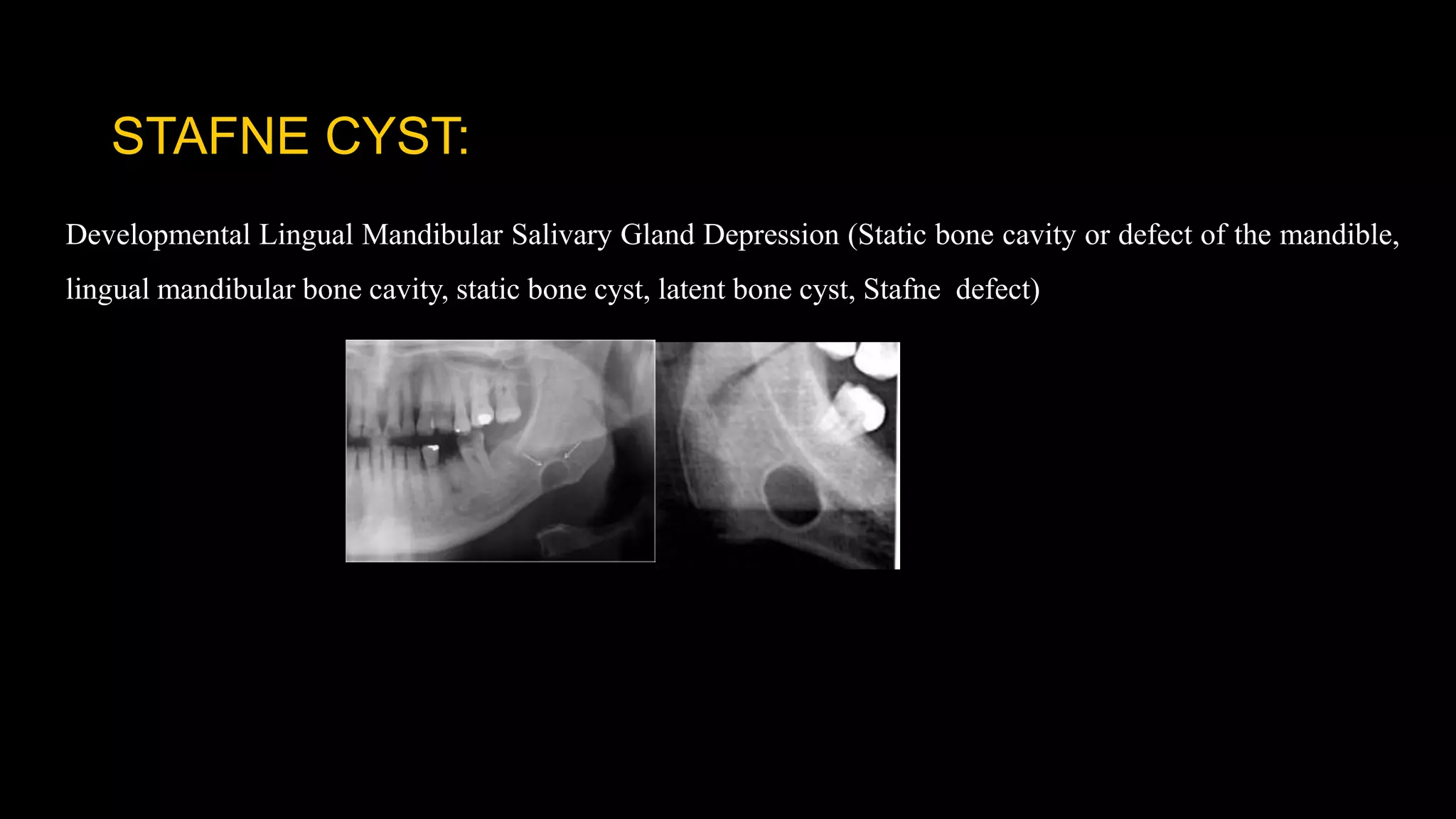
This document provides an overview of developmental disturbances of the jaws and teeth. It begins with introductions and terminology. It then discusses various developmental disturbances that can affect the jaws, such as agnathia, micrognathia, macrognathia, and clefts. Tooth disturbances covered include anomalies in size, number, morphology, structure, and position. Specific conditions discussed include microdontia, hypodontia, taurodontism, amelogenesis imperfecta, and dens invaginatus. Finally, the document examines some developmental cysts of the jaws, such as the nasopalatine duct cyst, median palatal cyst, and Stafne cyst. The conclusion thanks the reader.


















































































![[Pedo] restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/pedorestorativedentistry-210903140140-thumbnail.jpg?width=640&height=640&fit=bounds)