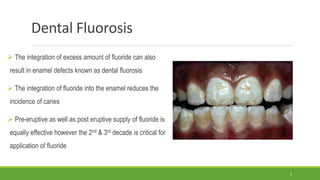
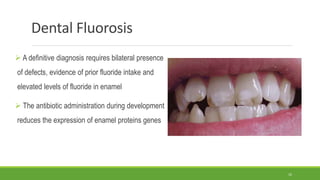
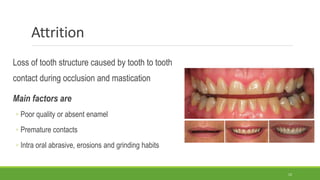
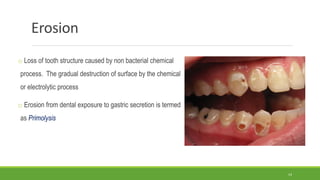
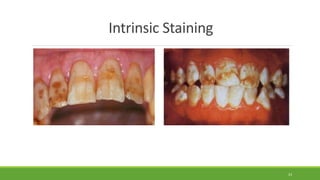
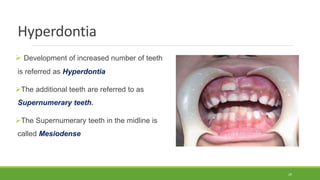
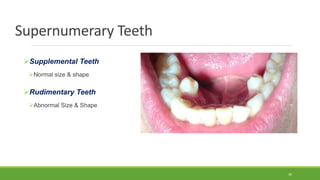
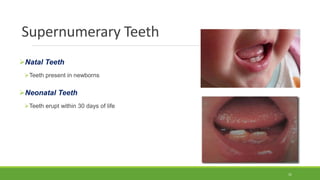
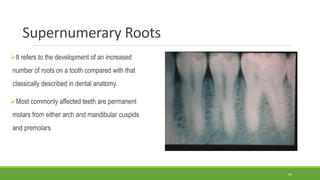
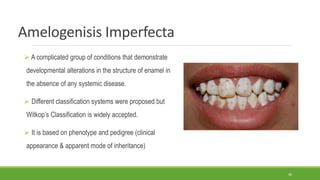
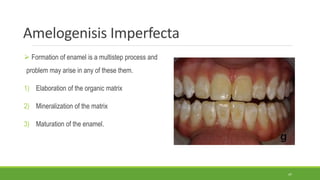
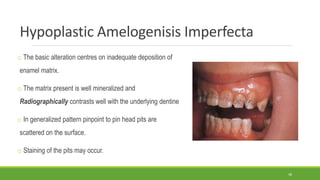
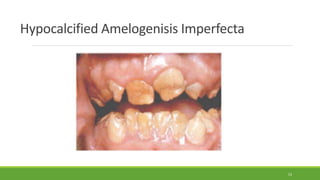
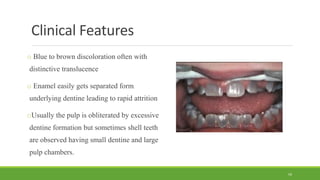
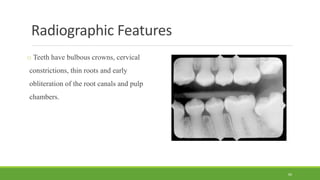
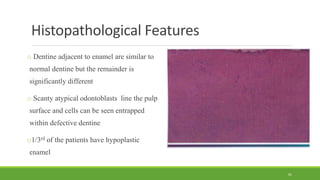
The document discusses various abnormalities and developmental alterations that can occur in teeth. It covers defects in enamel formation like enamel hypoplasia and fluorosis. It also discusses post-developmental structural loss through processes like attrition, abrasion, and erosion. Other topics include discoloration of teeth from extrinsic and intrinsic factors, localized disturbances in eruption, and developmental defects affecting tooth number, size, shape and structure. Specific conditions discussed in more depth include dentinogenesis imperfecta, amelogenesis imperfecta, and dental fluorosis. Treatment options for some of these conditions are also mentioned.



















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









