



![Stepwise excavation of caries :
Technique in which caries is removed in increments in two or
three appointments over a few months to a year rather than
removing the caries in one sitting [ in deep carious lesions ]
Each time caries is removed
Glass ionomer base is placed
which may contribute to mineralization, followed by a well
sealing temporary restoration](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-13-320.jpg)
![ Place a layer of Glass ionomer [or calcium hydroxide]
and restore the tooth with a provisional restoration
The seal provided by the restoration is very important
After 1-2 months remove the restoration and excavate
the remaining caries.
If any exposure then – direct pulp capping
Pulpotomy
pulpectomy
If no exposure - permanent restoration](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-16-320.jpg)
![ Success rate for Mechanical exposure > Carious exposures
Materials commonly used
•
•
MTA [Mineral Trioxide Aggregate]
Calcium hydroxide
These materials should be covered by a permanent
restoration with a good marginal seal](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-19-320.jpg)


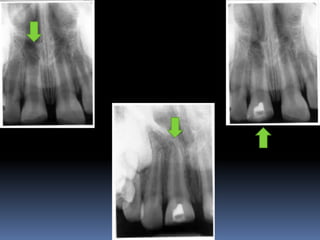
![Indications:
Exposed vital pulps in carious primary teeth
Exposed
permanent
vital
pulps
teeth
(to
in
carious
allow
immature
continued
root
development prior to NSRCT)
Traumatically exposed primary or permanent teeth
[mature or immature]
As an emergency procedure prior to NSRCT](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-25-320.jpg)

![Technique:
1. Anesthesia and rubber dam isolation
2. The inflamed pulp tissue is removed using a sharp round
bur in a high speed hand piece with water coolant for
superficial 2-3mm of pulp amputaion [Cvek pulpotomy]
3. Or removal of the entire pulp to the level of the canal
orifices using a large Spoon excavator
4. Hemorrhage is controlled by pressure on a cotton pellet
moistened with saline.
[ failure to achieve hemorrhage indicates pulpal inflammation]](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-37-320.jpg)

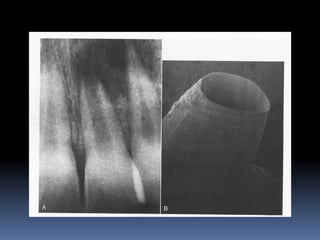
![APEXIFICATION
Induction of a calcific barrier or creation of an artificial barrier
across an open apex
Technique:
Local anesthesia and Rubber Dam isolation
Access cavity preparation and extirpation of the pulp
Working length is established slightly short of the apex [to
prevent injury to apical tissues]
Instrumentation and copius irrigation
Drying the canal and introducing MTA into the canal](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-41-320.jpg)
![ Packing MTA using endodontic pluggers or special
system like MAP SYSTEM [Micro Apical placement]
MTA acts as an artificial barrier against which Gutta
percha can be condensed.
Calcium hydroxide produces a biologic barrier but takes
longer time.](https://image.slidesharecdn.com/vtpstdntcopy-140120060742-phpapp02/85/Vital-Pulp-Therapy-42-320.jpg)


Vital pulp therapy aims to preserve healthy pulp tissue and includes procedures like indirect/direct pulp capping, pulpotomy, and apexification. The goal is to stimulate reparative dentin formation and maintain the tooth as a functional unit. Success depends on factors like the patient's age, pulp chamber size, bacterial contamination, and quality of the restoration. Indirect pulp capping involves stepwise caries removal and capping the remaining dentin layer, while direct capping places a material directly over an exposed pulp. Pulpotomy and apexification procedures are used to treat immature teeth and maintain root development.


































































































