Downloaded 556 times
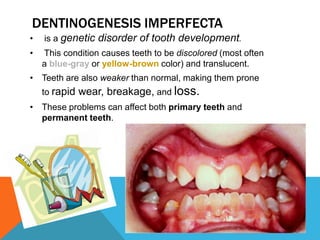
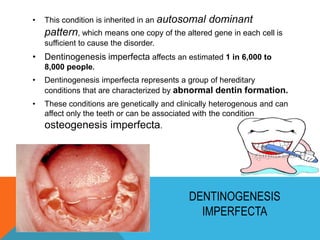

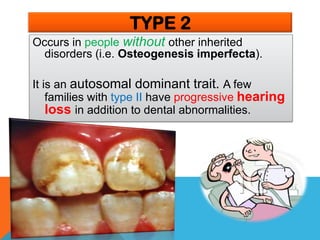


Dentinogenesis imperfecta is a genetic disorder that causes teeth to be discolored and translucent, as well as weaker and prone to breakage. It is caused by abnormal dentin formation and is inherited in an autosomal dominant pattern. The condition affects an estimated 1 in 6,000 to 8,000 people and can involve both primary and permanent teeth. Treatment focuses on bonding to strengthen enamel and make teeth appear whiter, as common cosmetic procedures are inappropriate due to the weakened state of the teeth.











































































































