Downloaded 458 times







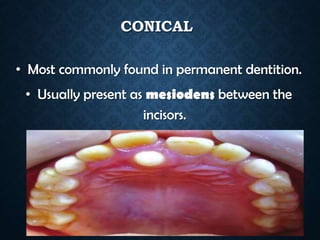












































This document summarizes various dental anomalies related to number, size, shape and structure of teeth. It describes conditions such as hypodontia, supernumerary teeth, microdontia, macrodontia, fusion, gemination, dens invaginatus and others. The causes, characteristics and classifications of these anomalies are discussed. Various hereditary conditions affecting dentin or enamel formation like dentinogenesis imperfecta, amelogenesis imperfecta, dentin dysplasia and odontodysplasia are also summarized.












































































