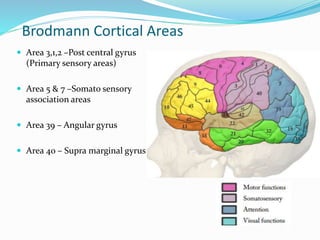
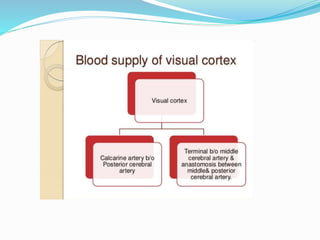
This document summarizes information about the parietal and occipital lobes of the brain. It discusses the anatomical structures, functions, and clinical effects of lesions to these areas. Key points include that the parietal lobe is involved in somatosensory processing, visual-spatial functions, and language abilities depending on lateralization. Lesions can cause syndromes like neglect or Gerstmann syndrome. The occipital lobe is the visual processing center and lesions can result in visual field deficits or conditions like Balint's syndrome.


![CLINICAL EFFECTS OF PARIETAL LOBE LESIONS
Either hemi sphere
• CORTICAL SENSORY SYNDROMES
• TOPOGRAPHICAL DISORIENTATION
• VISUOSPATIAL DIFFICULTIES
HEMINEGLECT
• Total hemi anesthesia with large acute lesion of Parietal
lobe.white matter
Mild hemi paresis, unilateral muscular atrophy in children,
hypotonia, poverty of movements, hemiataxia
Homonymous hemianopia [incongruent or congruent],
Neglect of the opposite isde of external space](https://image.slidesharecdn.com/parietaloccipitallobes-141117075453-conversion-gate01/85/Parietal-occipital-lobes-13-320.jpg)






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
