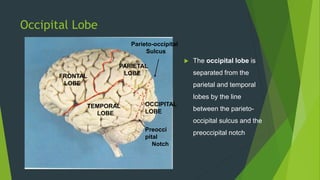
The occipital lobe is the visual processing center of the brain. It contains the primary visual cortex and several secondary visual cortices. Occipital tumors can cause a variety of visual symptoms like visual field defects, cortical blindness, visual hallucinations, or visual agnosia. On examination of patients with occipital tumors, doctors often find homonymous visual field defects, papilledema or optic atrophy, and motor or speech disturbances on the contralateral side of the body.




























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












