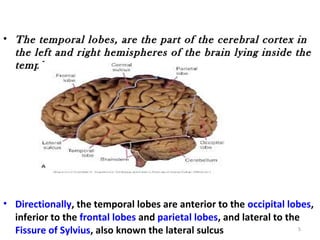
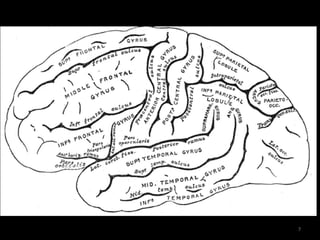
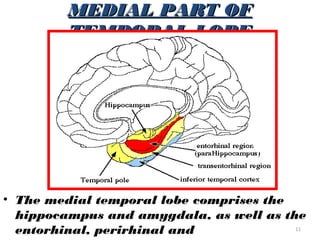
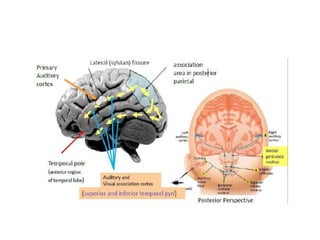
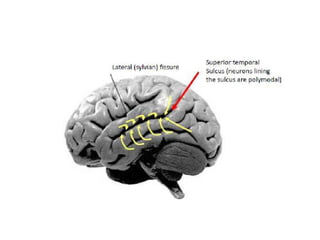
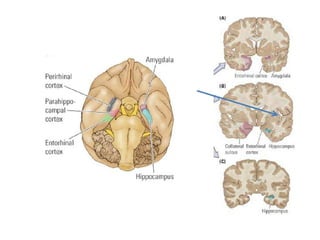
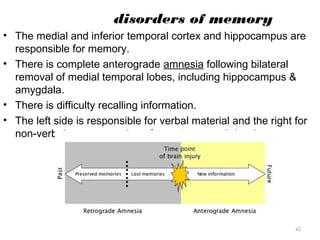
The temporal lobes are located inside the temples on both sides of the brain. They are divided into superior, middle, and inferior temporal lobes. The temporal lobes are involved in auditory processing, language comprehension, visual recognition, memory formation, and emotional processing. Disorders of the temporal lobes can cause issues with auditory and visual perception, attention, memory, language, personality, and behavior. The amygdala and hippocampus, located within the medial temporal lobes, are important for processing emotions and forming memories.