Downloaded 460 times

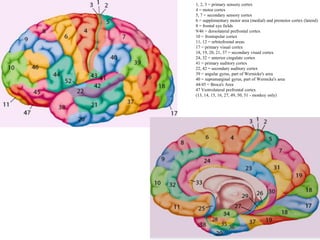
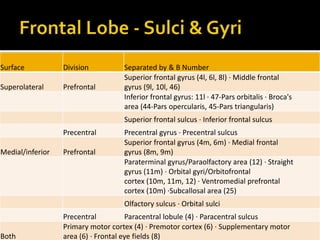
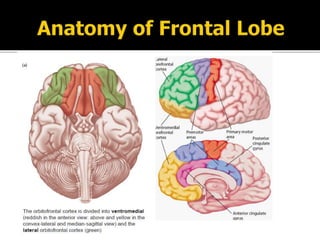
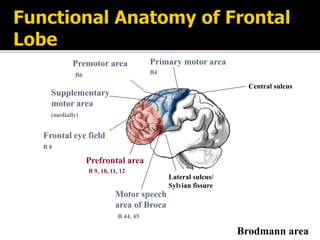
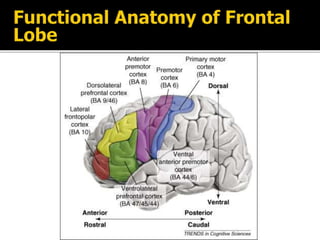
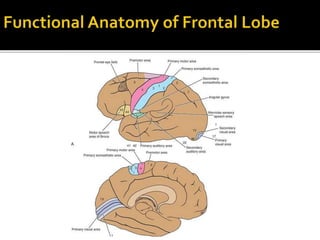
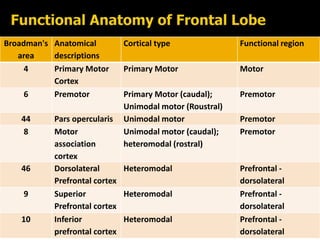
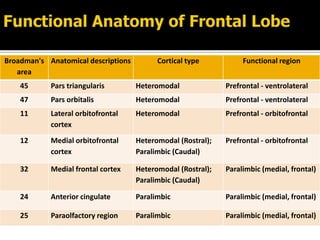
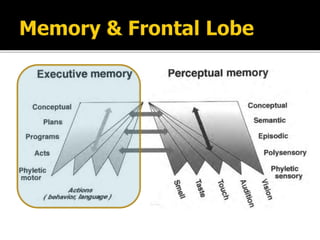
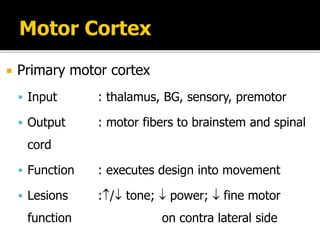
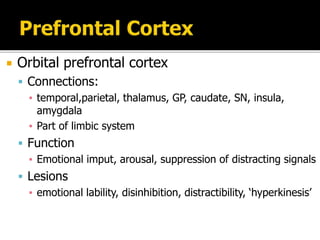
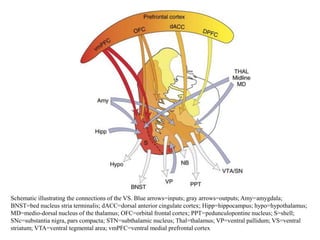
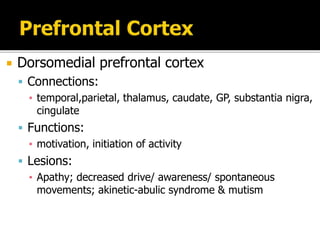
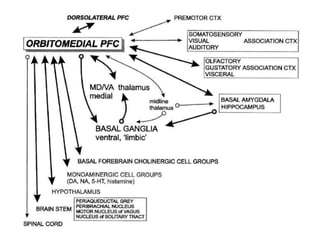
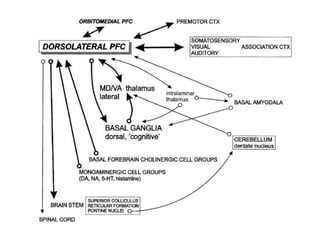
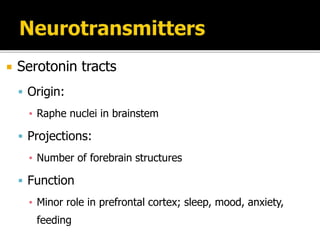
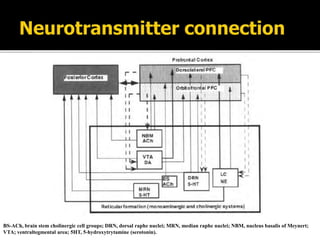
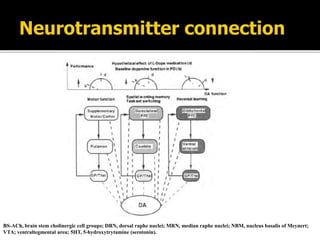
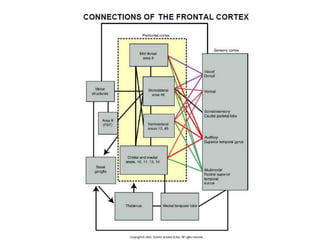
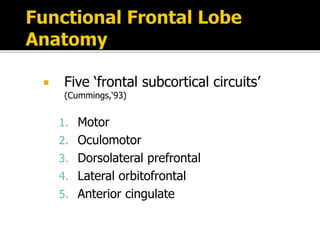
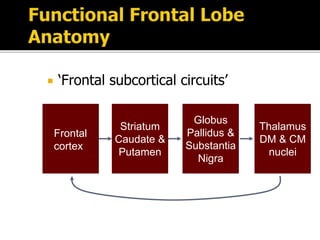
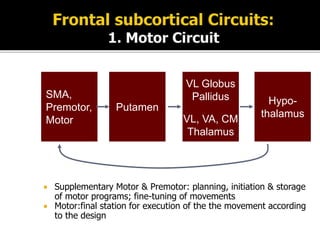
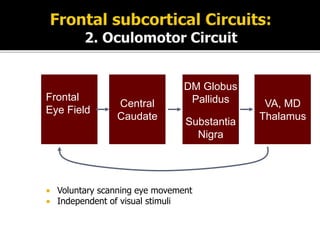
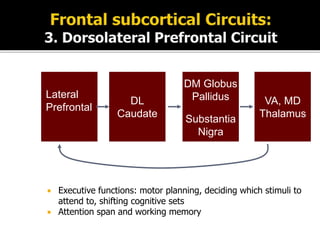
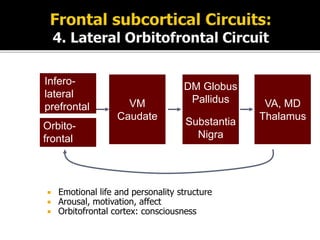
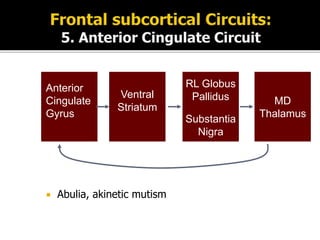
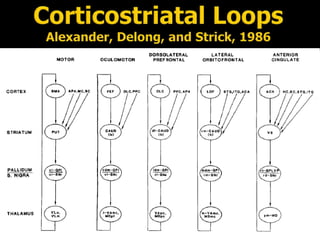
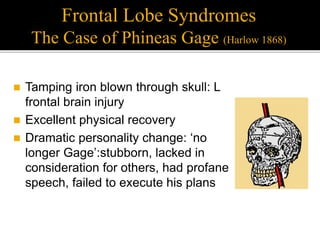


The document discusses the anatomy and functional areas of the frontal lobes, including the motor cortex, premotor cortex, dorsolateral prefrontal cortex, orbitofrontal cortex, and their connections. It also examines frontal lobe circuits and the neurotransmitters that project to the frontal lobes. Common frontal lobe syndromes and deficits associated with lesions to different frontal areas are described.