Downloaded 85 times




![Nephrotic syndrome [full]](https://image.slidesharecdn.com/nephroticsyndromefull-161026190255/85/Nephrotic-syndrome-full-34-320.jpg)

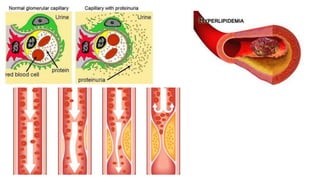
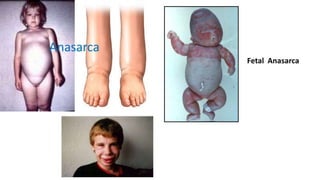
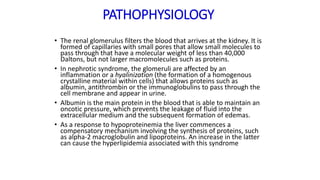
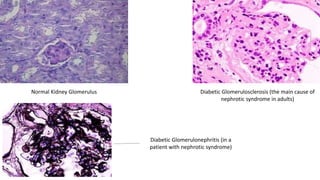
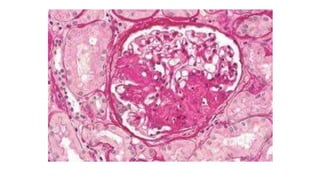
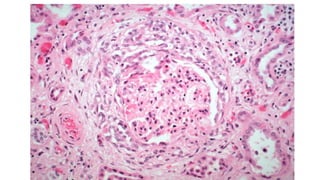
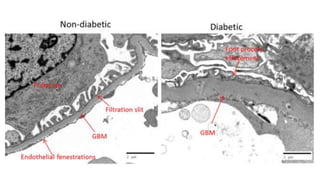
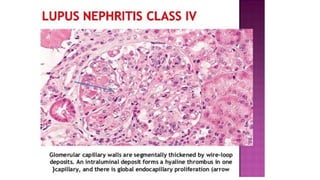
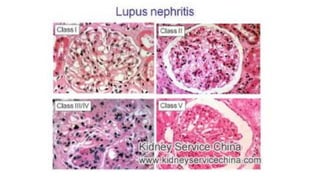
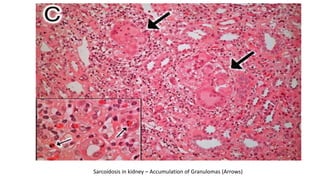
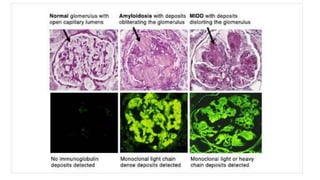
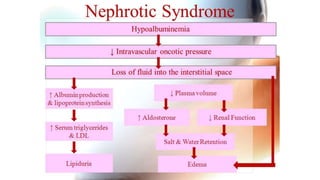
Nephrotic syndrome is a kidney disorder characterized by significant proteinuria, hypoalbuminemia, hyperlipidemia, and edema, resulting from damage to the renal glomeruli. It can be classified as primary (e.g., minimal change disease) or secondary (e.g., diabetic nephropathy, systemic lupus erythematosus) depending on the underlying cause. The condition leads to various complications, including increased risk of thrombosis and altered fluid distribution due to low protein levels in the blood.








































































![Hepatitis [full]](https://cdn.slidesharecdn.com/ss_thumbnails/hepatitisfull-161102103834-thumbnail.jpg?width=640&height=640&fit=bounds)























