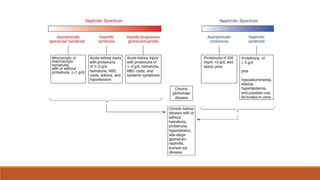
The document discusses nephrotic syndrome and nephritic syndrome. It covers:
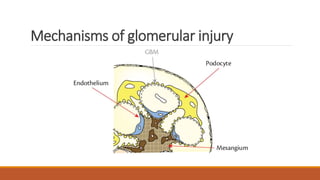
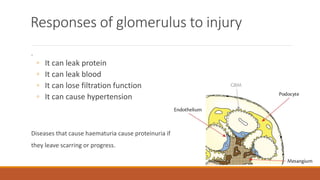
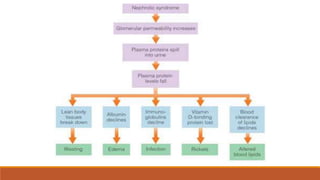
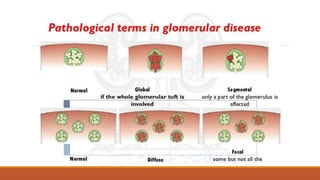
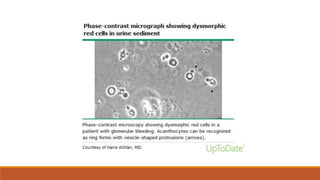
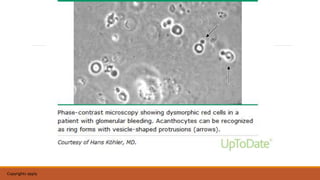
- Mechanisms of glomerular injury including proteinuria, hematuria, loss of filtration function, and hypertension.
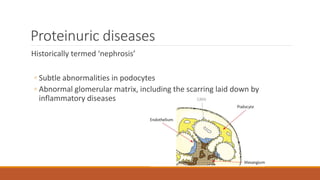
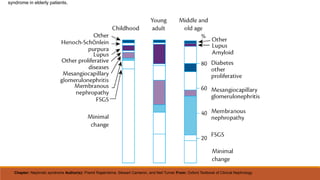
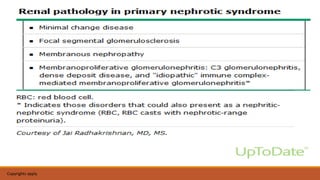
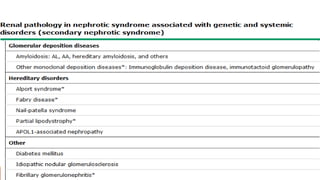
- Causes of nephrotic syndrome including minimal change disease, membranous nephropathy, and focal segmental glomerulosclerosis which often involve podocyte dysfunction.
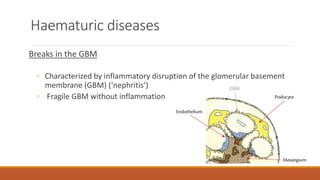
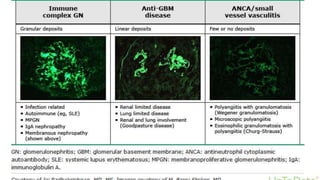
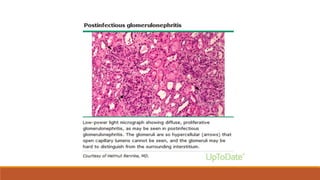
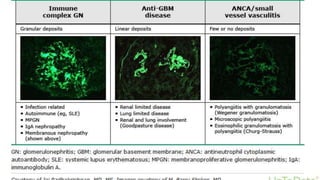
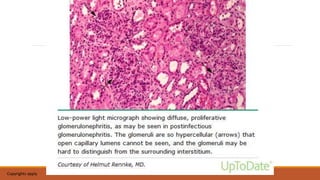
- Causes of nephritic syndrome include inflammatory diseases that break the glomerular basement membrane such as post-streptococcal glomerulonephritis.






































![Nephrotic syndrome [full]](https://cdn.slidesharecdn.com/ss_thumbnails/nephroticsyndromefull-161026190255-thumbnail.jpg?width=640&height=640&fit=bounds)



















