

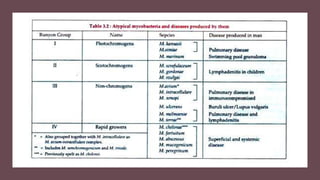
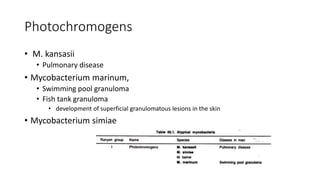
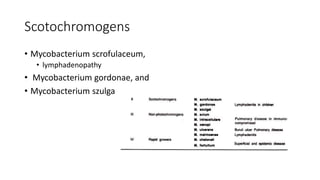
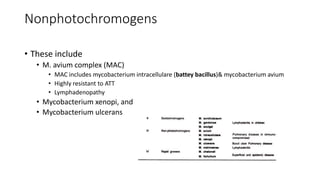


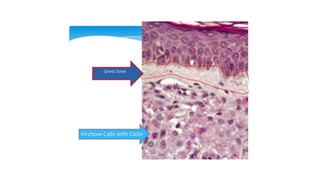

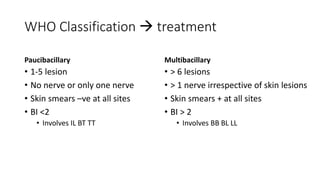
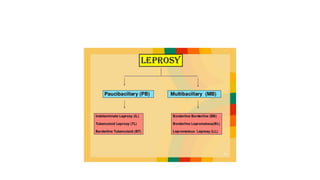





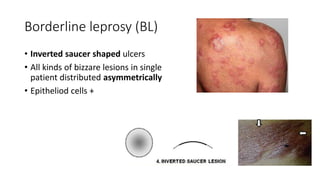
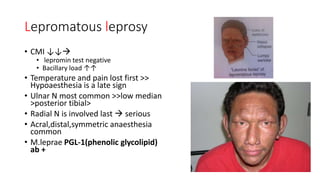
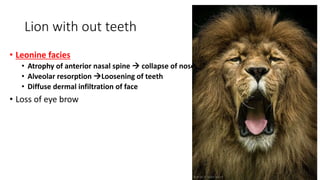


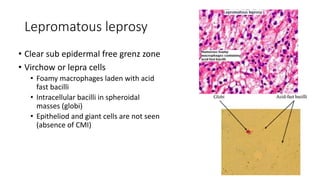
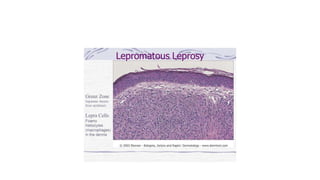
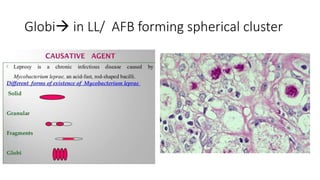

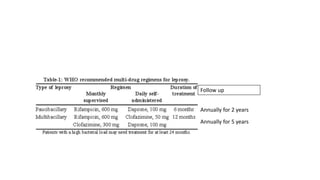



- Atypical mycobacteria include nontuberculous mycobacteria found in the environment that can cause disease in humans under certain conditions. - Mycobacterium leprae causes leprosy (Hansen's disease), with a spectrum of clinical manifestations depending on immune response from tuberculoid to lepromatous leprosy. - Diagnosis involves skin smears and biopsy showing acid-fast bacilli. Treatment is multidrug therapy including dapsone, rifampin, and clofazimine.











![[Micro] mycobacterium tuberculosis](https://cdn.slidesharecdn.com/ss_thumbnails/knwspassdmixhofx5ycy-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)










































































