This document provides an overview of leprosy (Hansen's disease):
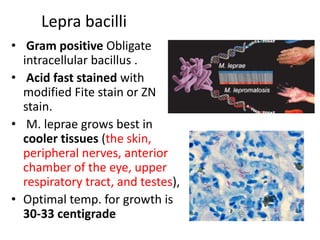
- It is caused by Mycobacterium leprae and mainly involves the peripheral nerves and skin. It can also involve other organs like the mouth, eyes, bones, and testes.
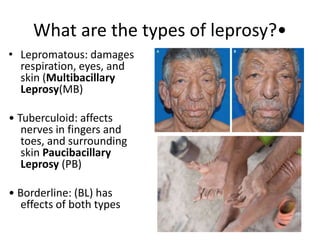
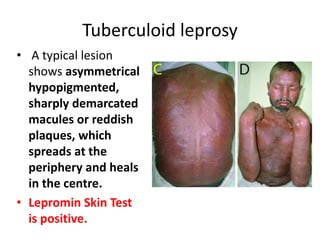
- Leprosy exists in several forms along a spectrum from tuberculoid leprosy to lepromatous leprosy. It is transmitted through droplets from the nose and mouth during close and frequent contact with untreated cases.
- Diagnosis involves clinical symptoms, skin smears, skin biopsies, and nerve biopsies to look for acid-fast bacilli and determine bacterial load and immune response patterns. There is