



![Causes of babinkis sign
• UMN disease
• Infants < 1 year of age
• d/t incomplete myelination
• Comatosed pateints
• Post ictal stage of epilepsy
• Deep sleep
• GA
• ECT ]](https://image.slidesharecdn.com/plantarreflex-200121063031/75/Plantar-reflex-15-2048.jpg)
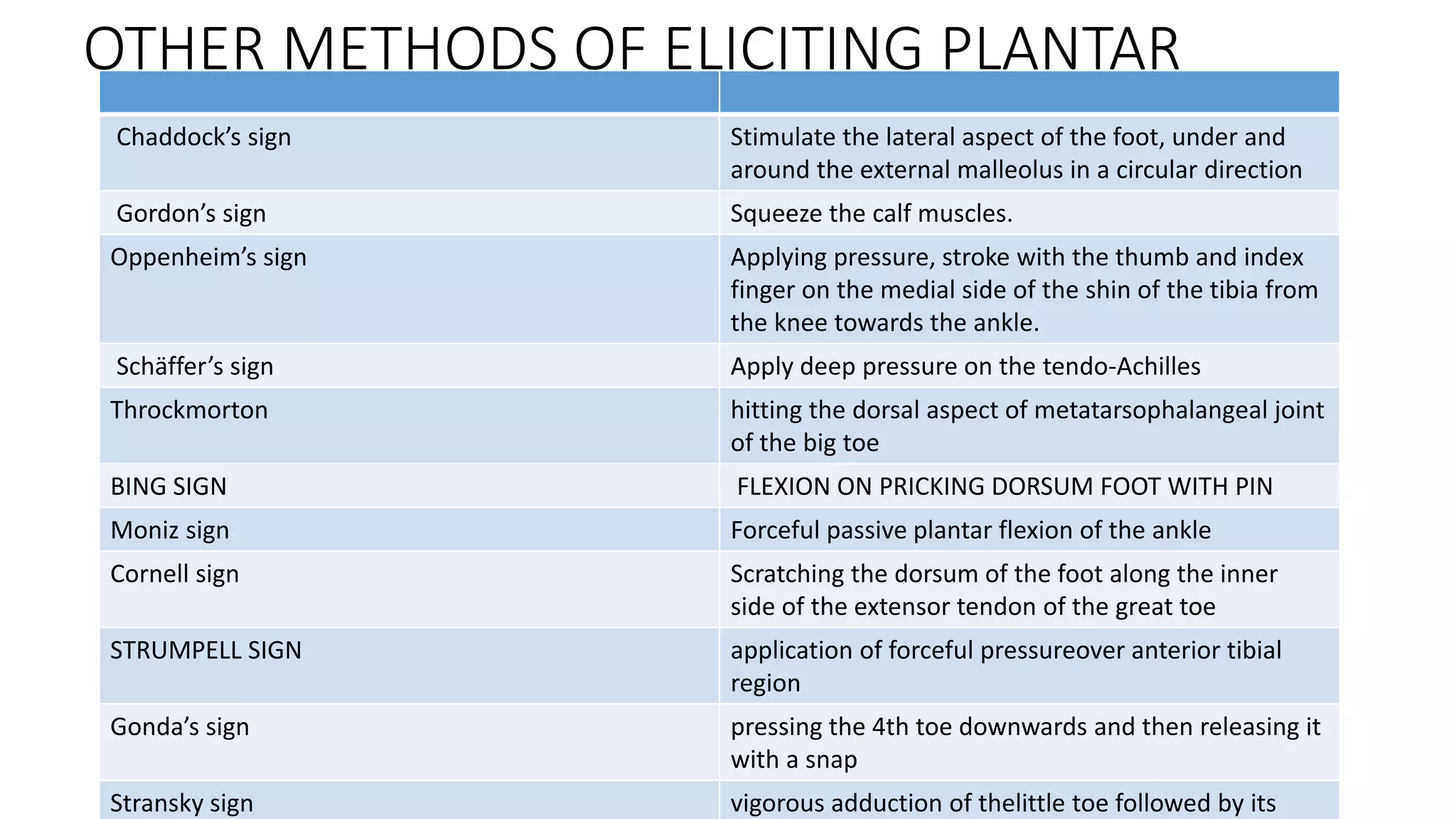

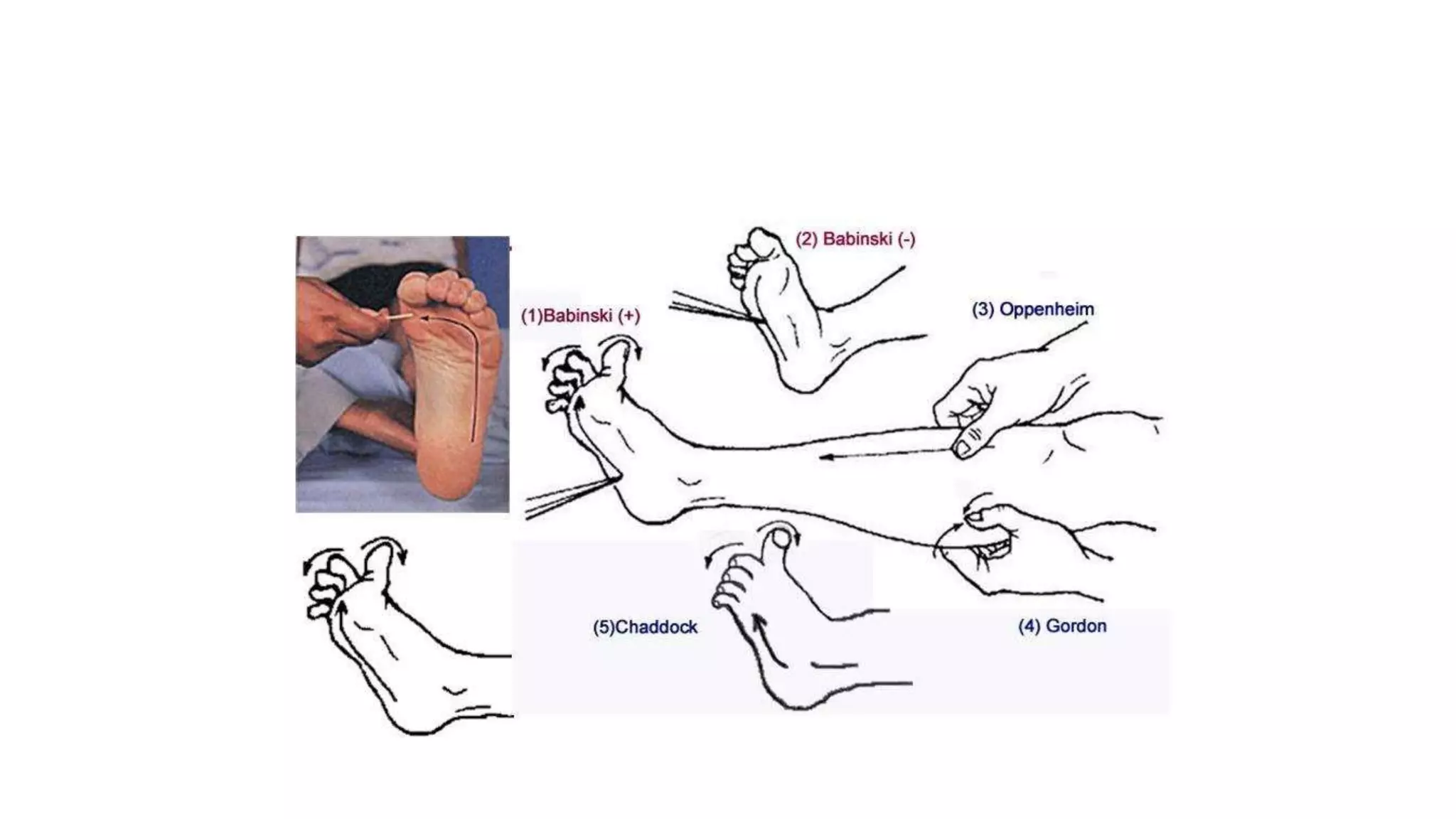

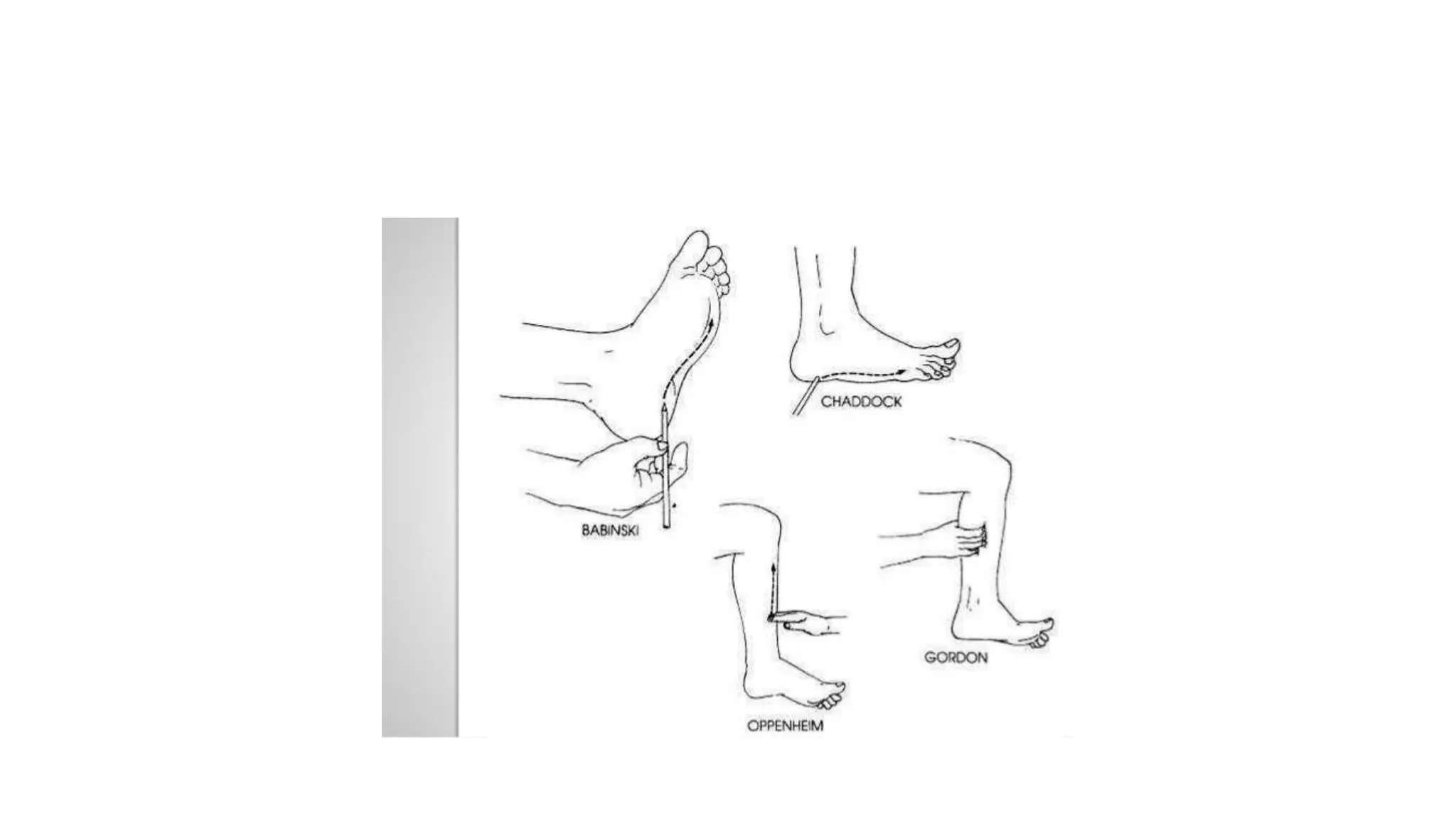
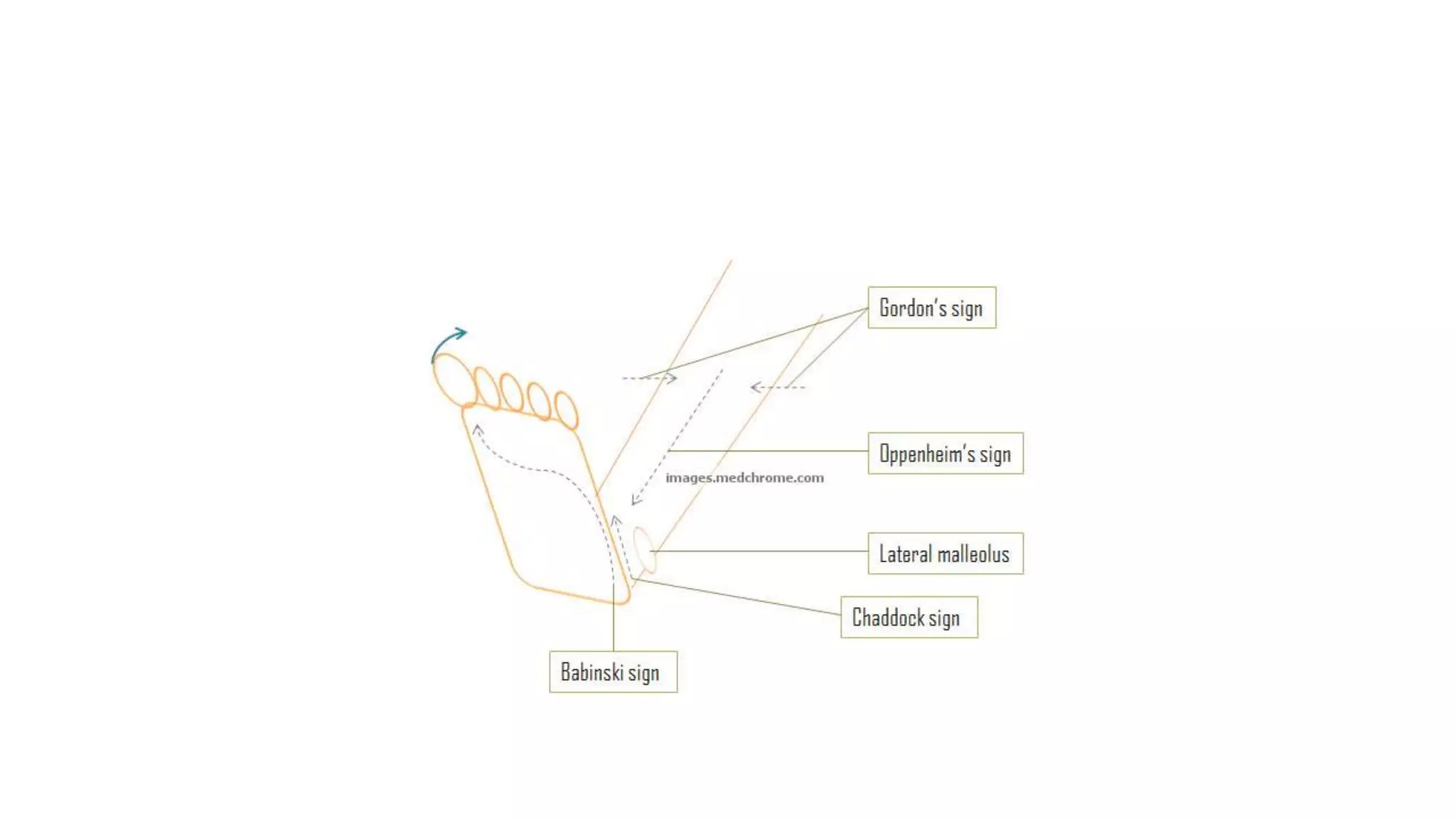






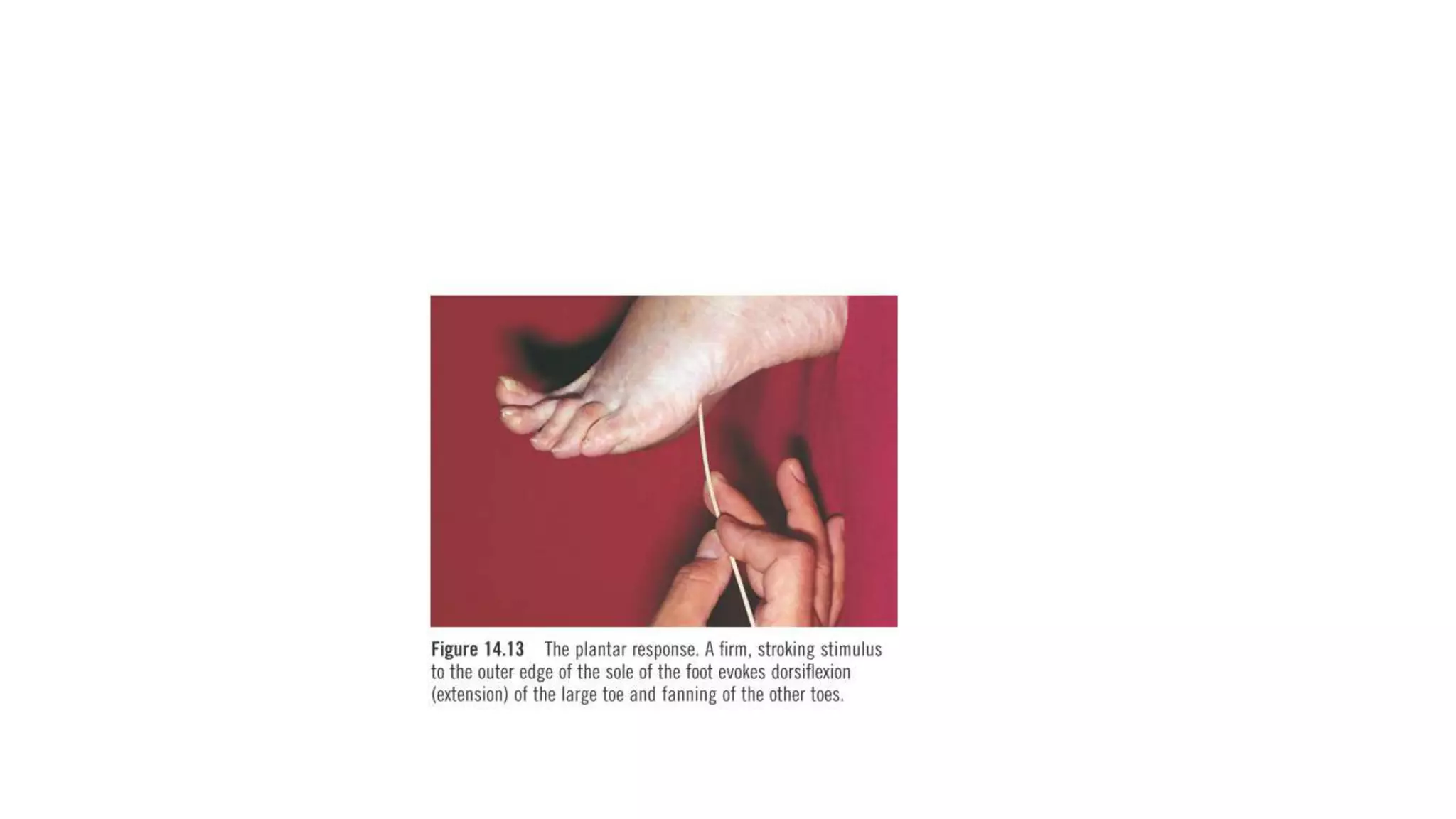
The plantar reflex is an important superficial reflex that involves polysynaptic pathways. A normal plantar reflex results in flexion of the toes when the sole is scratched, while an extensor plantar response (Babinski's sign) involves dorsiflexion of the great toe and fanning of the other toes and suggests corticospinal tract dysfunction. There are several methods to elicit the plantar reflex and variations in responses provide information about neurological conditions.