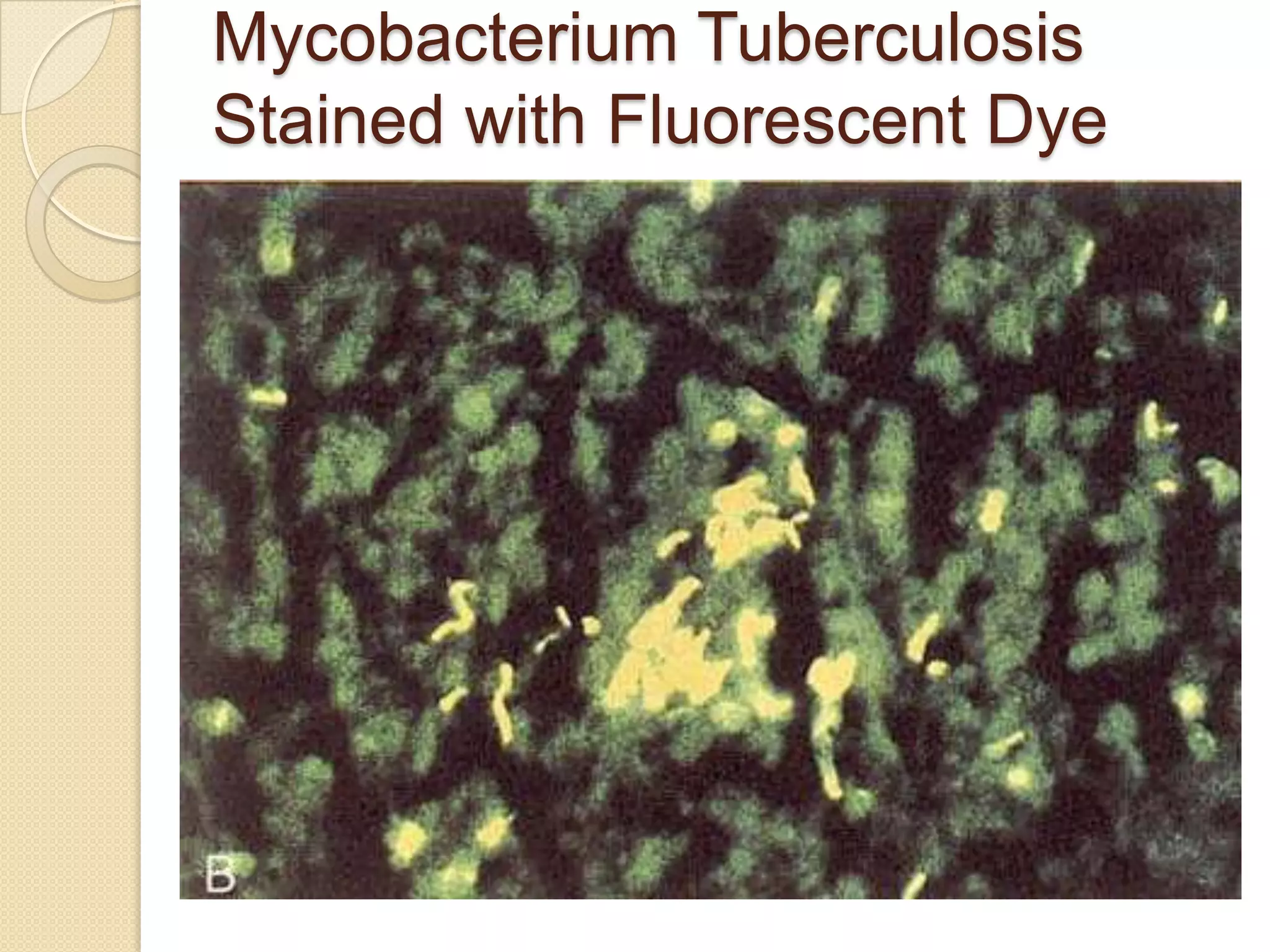
1. Mycobacterium is a genus of bacteria that includes M. tuberculosis and M. leprae, which are the causes of tuberculosis and leprosy, respectively.
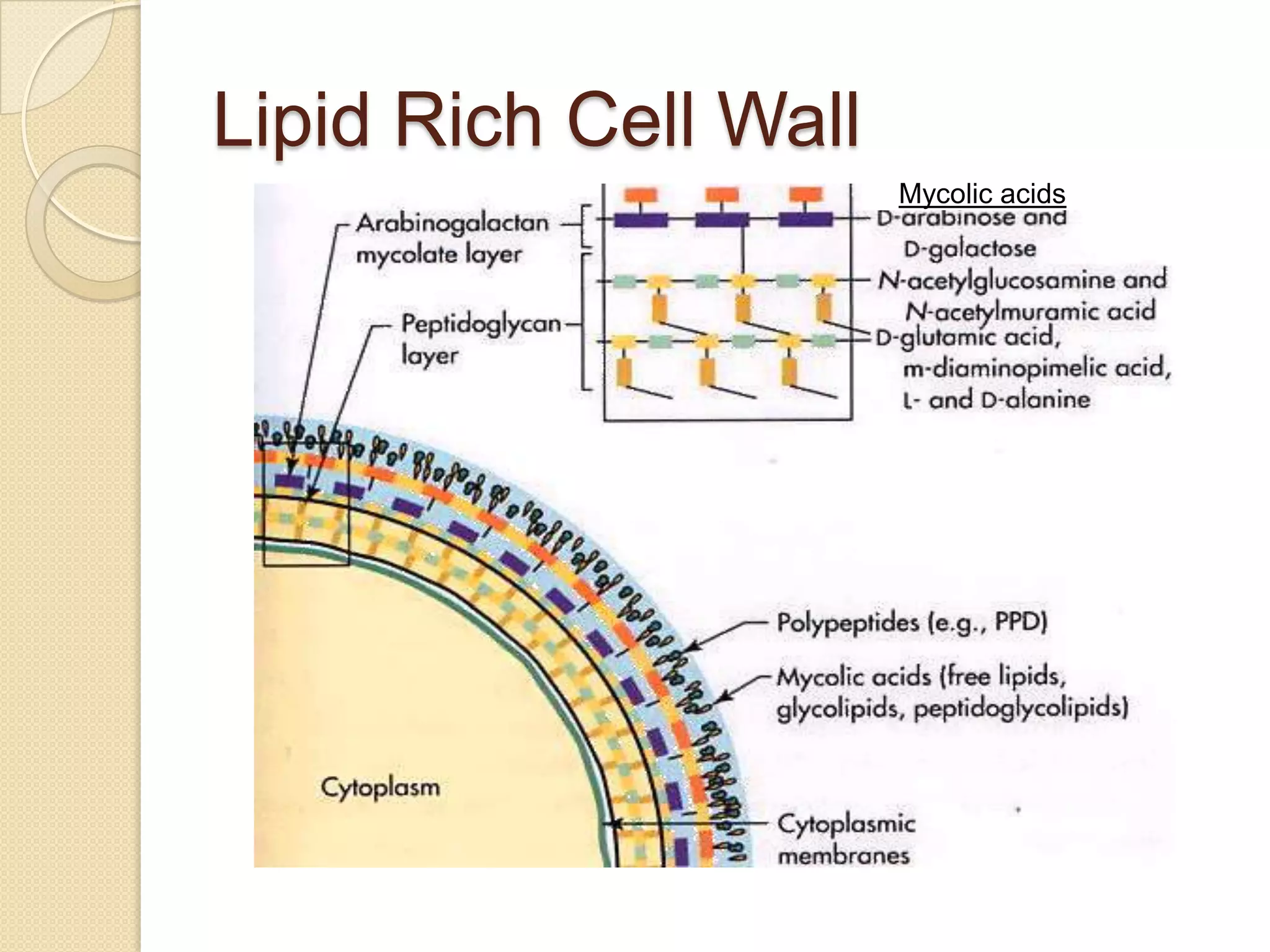
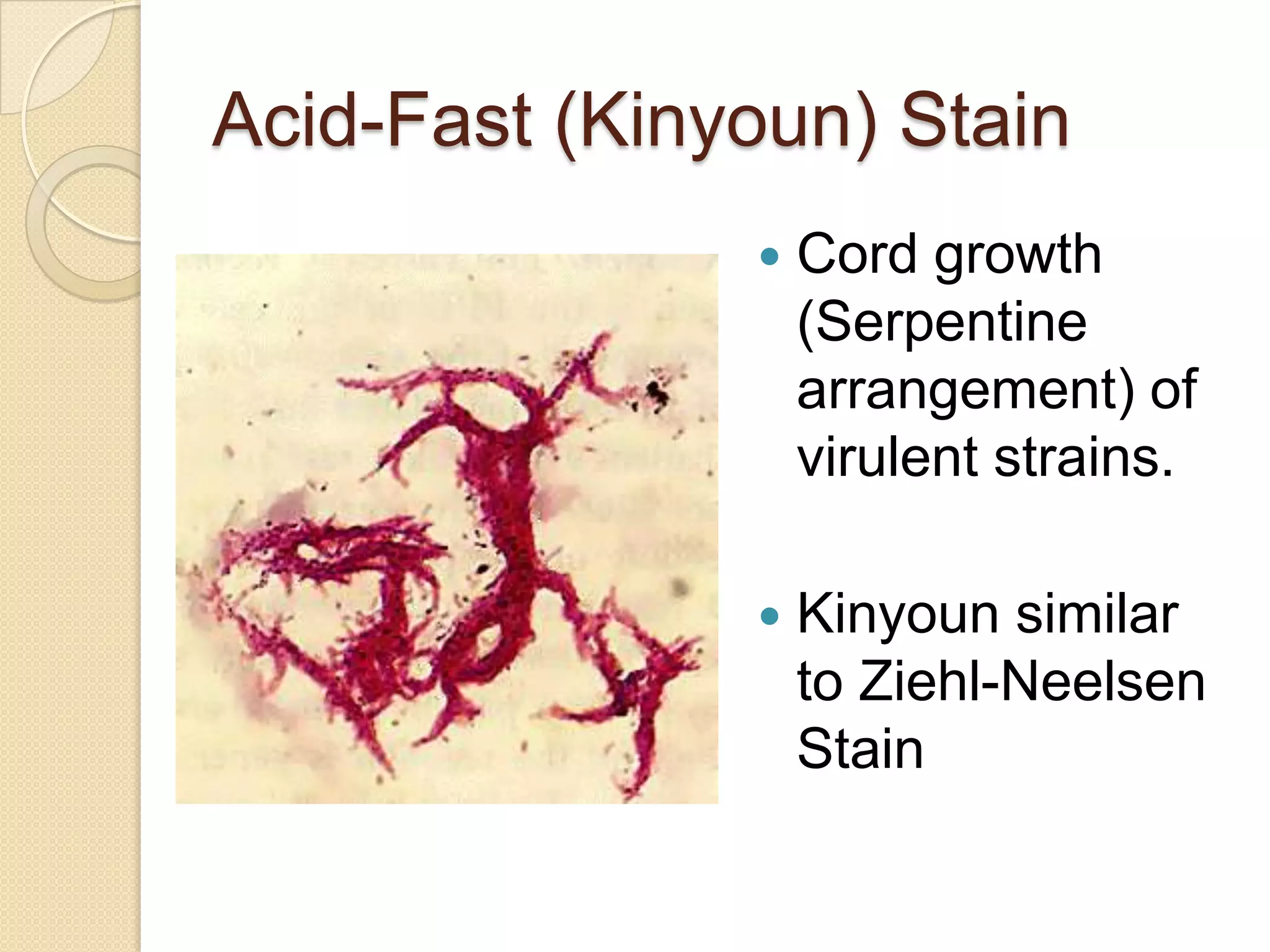
2. These bacteria have an acid-fast staining pattern and lipid-rich cell walls that make them resistant to disinfectants and antibiotics.
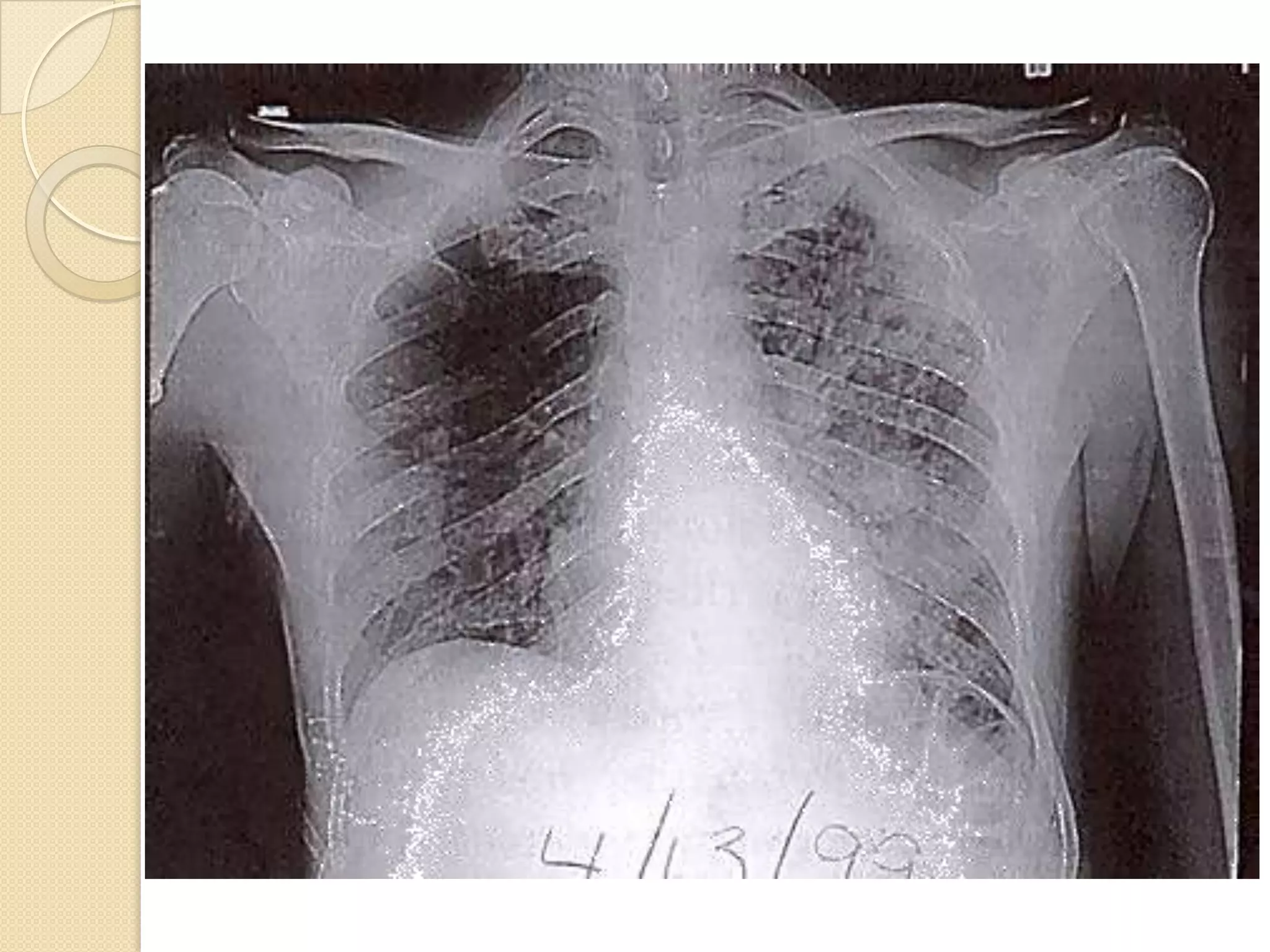
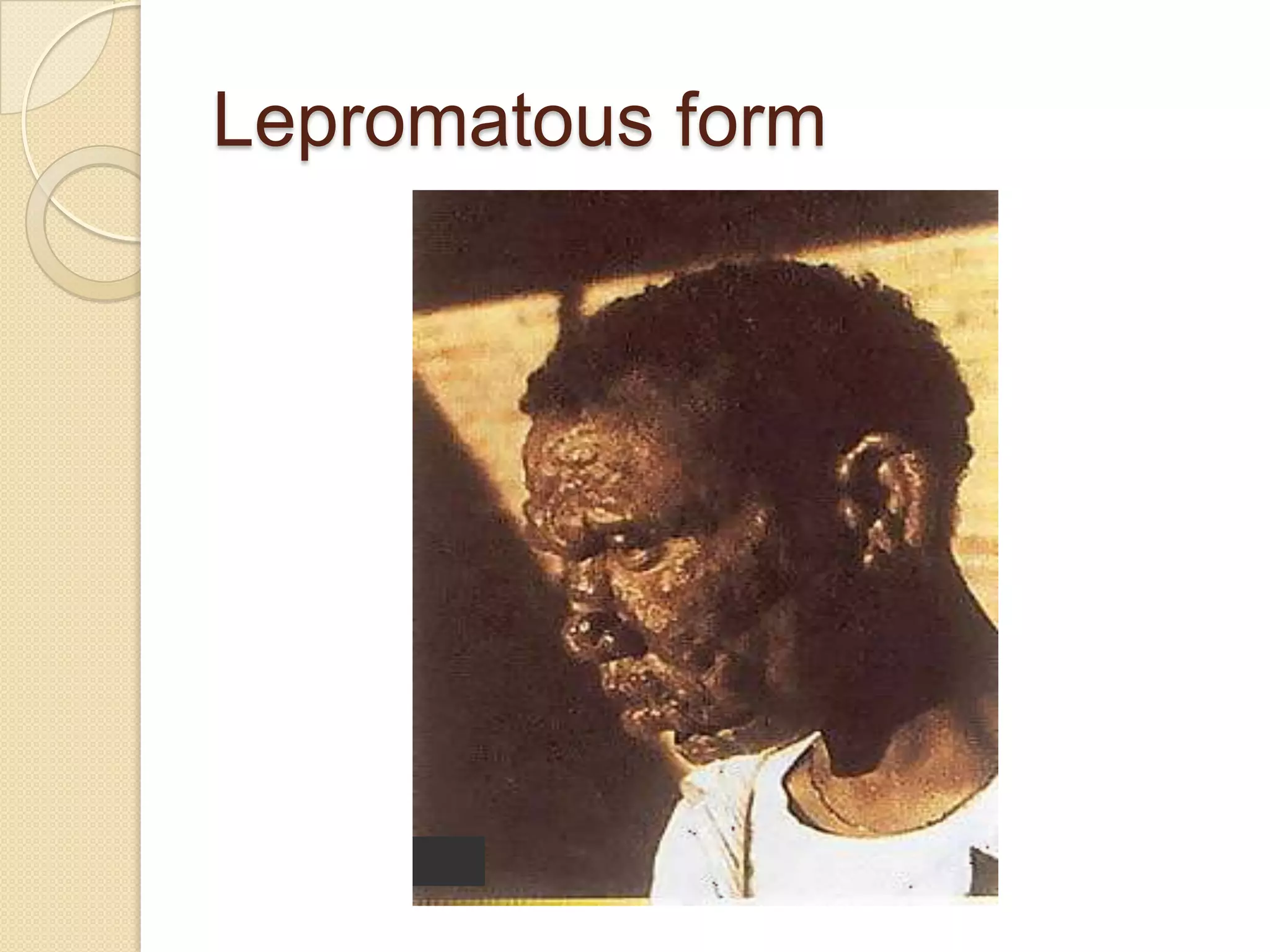
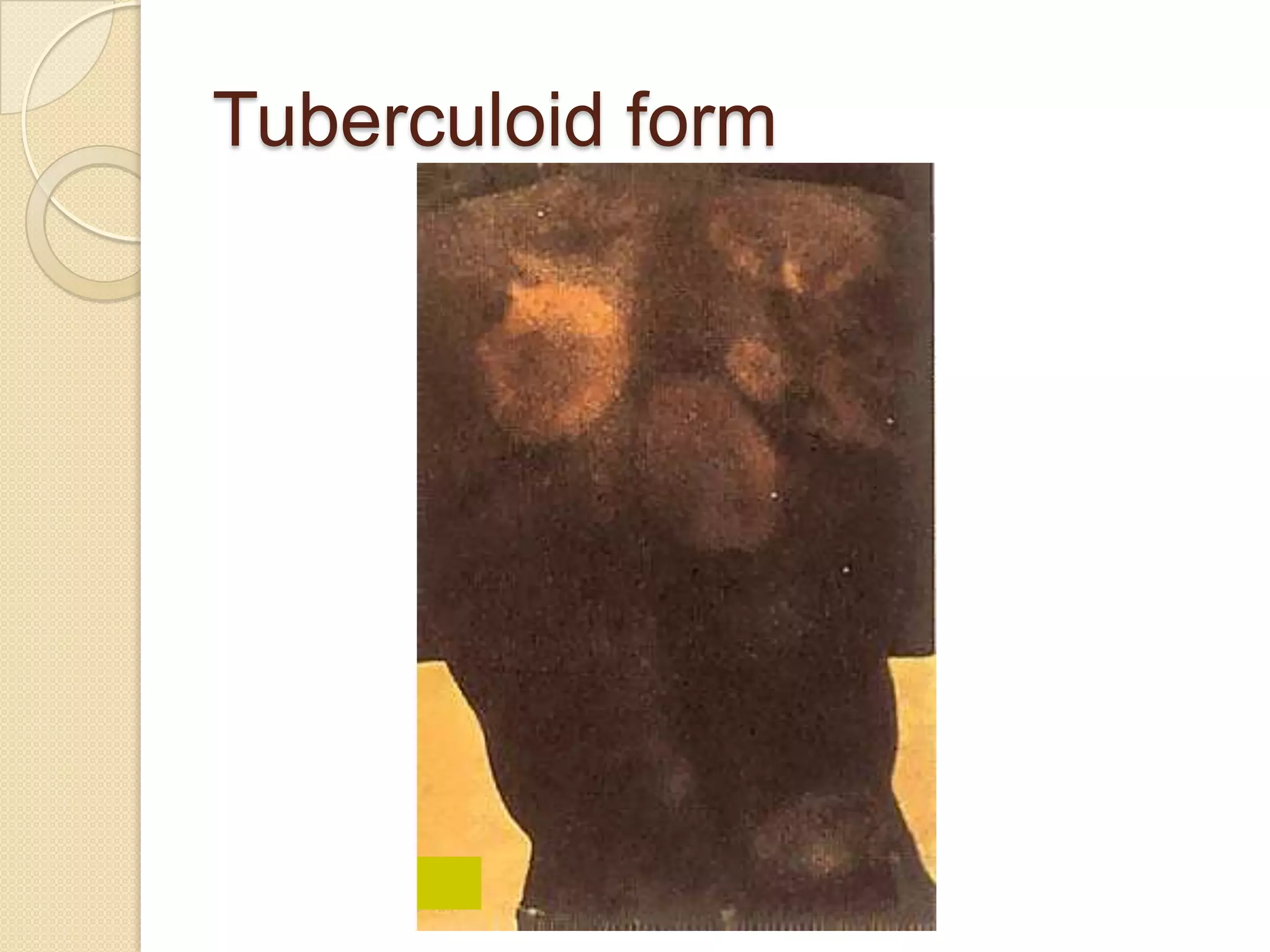
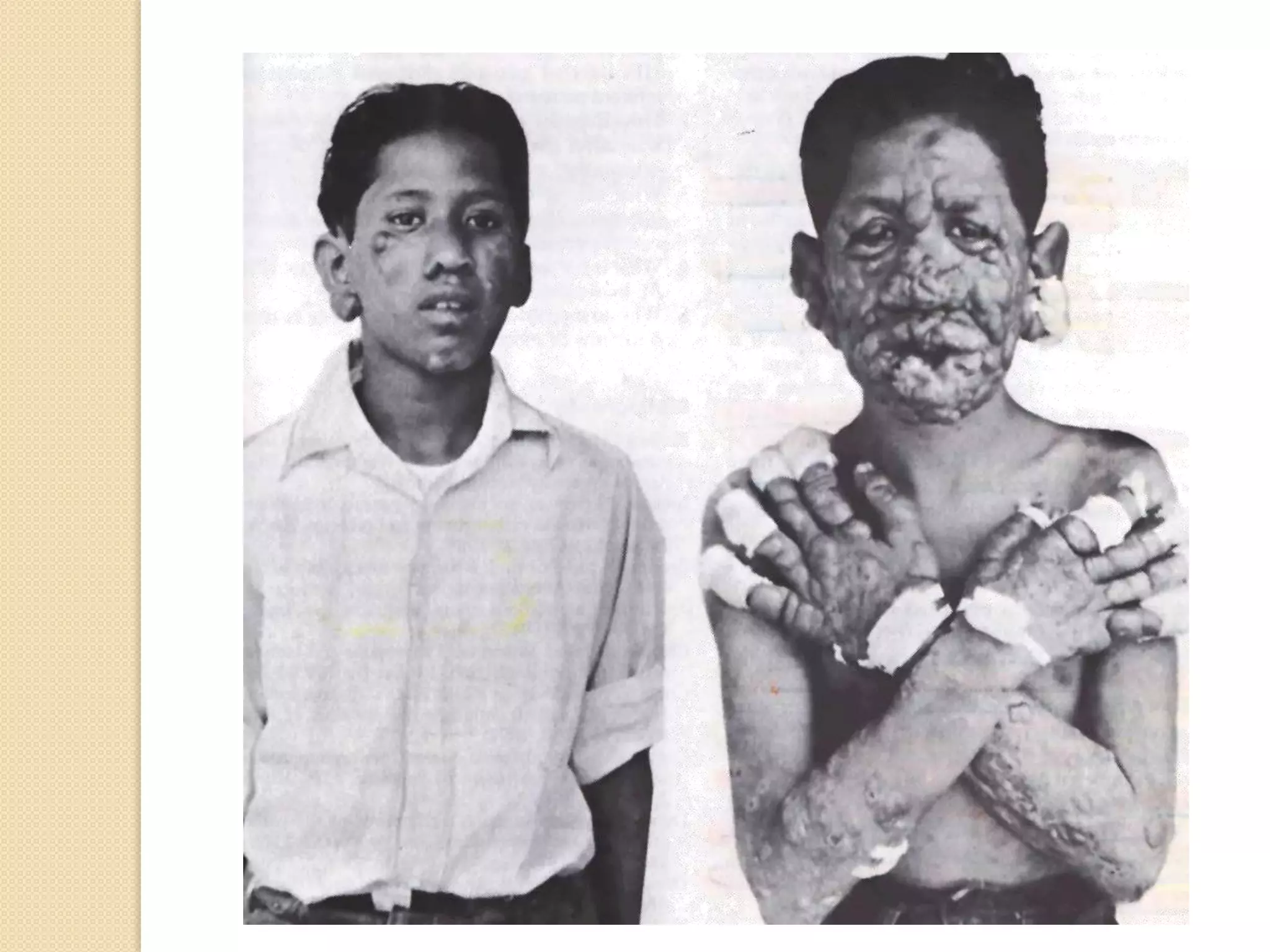
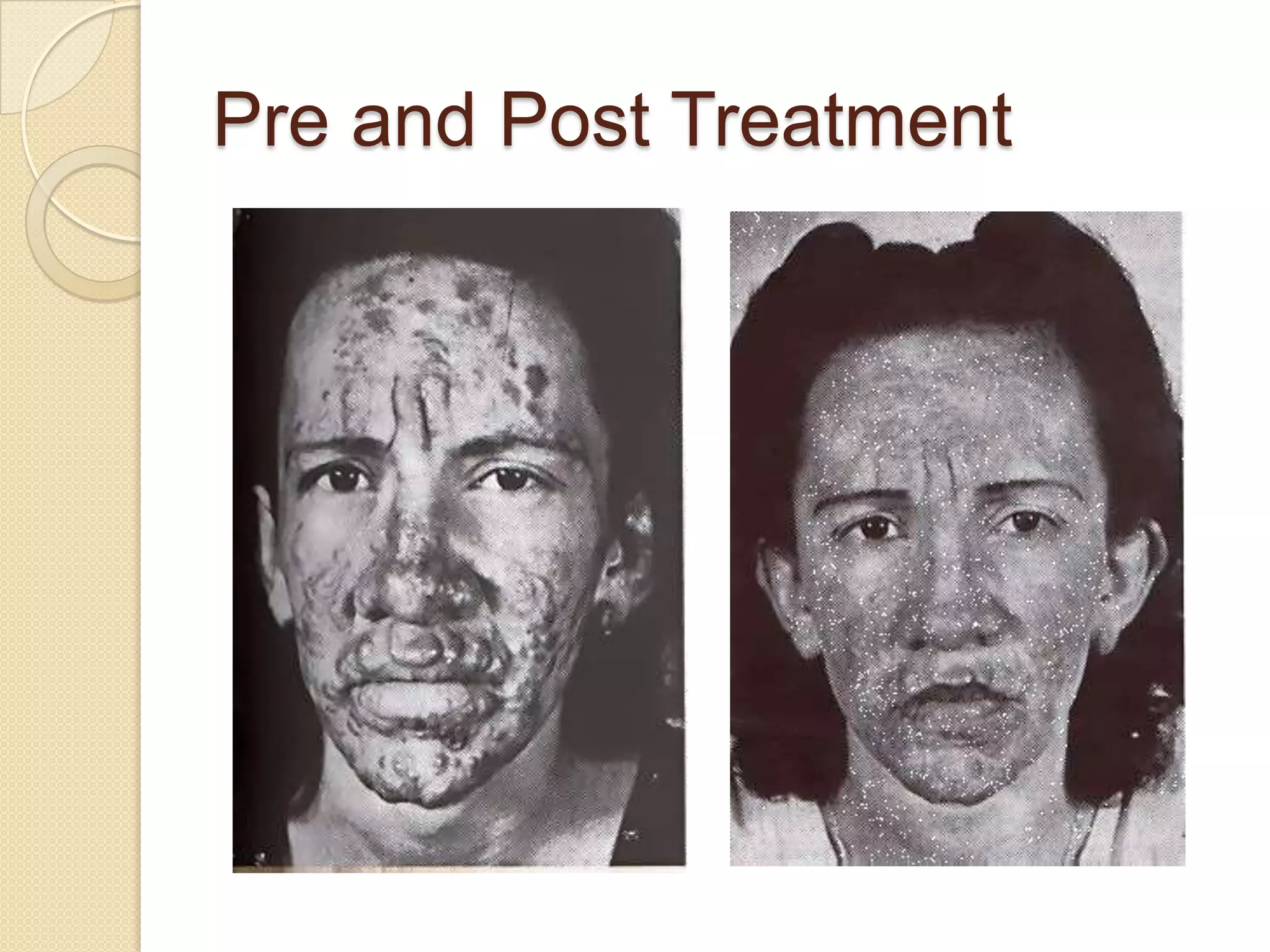
3. M. tuberculosis spreads through the air and causes pneumonia and cavitary lesions in the lungs, while M. leprae spreads through skin lesions and can cause disfigurement if untreated.