The document discusses guidelines and recommendations for weaning patients from mechanical ventilation and discontinuing ventilator support. Some key points covered include:
- Weaning involves gradually reducing ventilatory support as a patient's condition improves to avoid complications of prolonged ventilation.
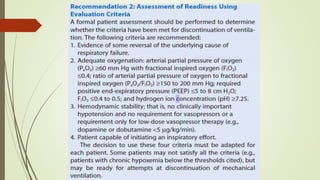
- Readiness for weaning depends on recovery from the underlying medical issues, overall clinical condition, and psychological state.
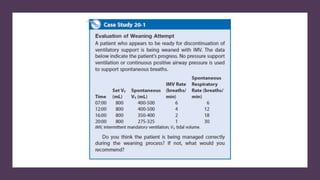
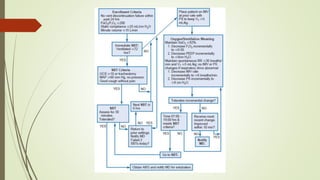
- Spontaneous breathing trials are recommended to assess a patient's ability to breathe independently without ventilator support.
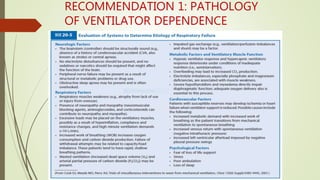
- Factors like ventilator mode, oxygen needs, airway protection, and non-respiratory medical conditions must be considered during the weaning process.
- Protocols and guidelines aim to standard































![Dual controlled modes of mechanical ventilation [onarılmış]](https://cdn.slidesharecdn.com/ss_thumbnails/dualcontrolledmodesofmechanicalventilationonarlm-151116121024-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)








































