1) The document discusses various physiologic variables that can predict a patient's readiness to be weaned from a mechanical ventilator, including the rapid shallow breathing index, maximal inspiratory pressure, and compliance.
2) It contrasts approaches to weaning patients such as a spontaneous breathing trial using T-piece trials or low levels of pressure support, and describes criteria for indicating a successful spontaneous breathing trial.
3) Common reasons for weaning failure include respiratory failure that has not improved, organ system dysfunction, low oxygenation or ventilation status, and lack of an intact airway protective mechanism.



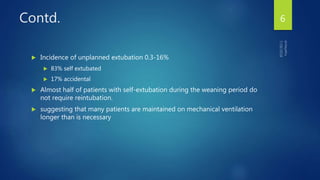











![Integrative indices
Weaning failure is usually multifactorial; single measures tend to be unreliable.
Indices that integrate several physiologic mechanisms were developed in an attempt
to further improve the accuracy of prediction.
The CROP index =[Cdyn x MIP x (PaO2 ÷ PAO2)] ÷ Respiratory Rate
CROP index >13 mL/breath per min is generally considered to predict weaning
success
weaning index = PTI x (VE40 ÷ VTsb)
An index <4 units per minute is generally considered to predict weaning success.
Integrative weaning index: [(Cst,rs)*SaO 2 ] / [f/VT],
An IWI ≥25 ml/cm H 2 O/breaths/min/liter predicted successful weaning with a
sensitivity and specificity of 0.97 and 0.94, respectively
Limitation is difficulty of measuring Cst,rs in spontaneously breathing pts
19](https://image.slidesharecdn.com/weaning-180718141339/85/mechanical-ventilation-Weaning-predictors-19-320.jpg)
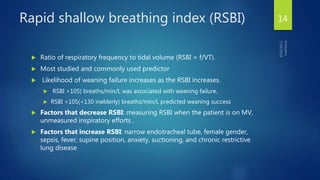
![Contd.
Inspiratory effort quotient (IEQ) = [(0.75VT/Cdyn) x (TI/TTOT)] / MIP,
where VT is the tidal volume, Cdyn is the dynamic compliance, TI is the inspiratory
time, TTOT is time of the respiratory cycle, and MIP is the maximal inspiratory
pressure.
An IEQ >0.15 has been suggested as the fatiguing threshold that
predicts weaning failure
20](https://image.slidesharecdn.com/weaning-180718141339/85/mechanical-ventilation-Weaning-predictors-20-320.jpg)