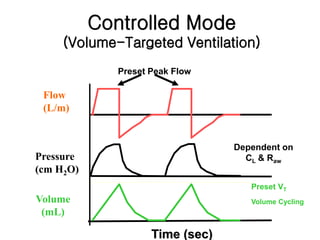
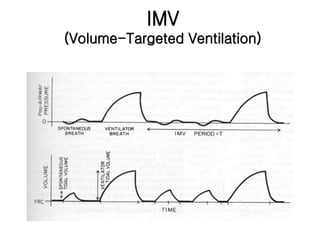
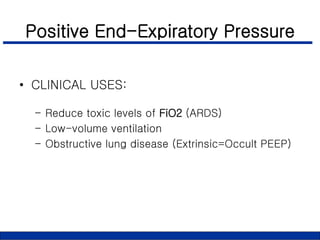
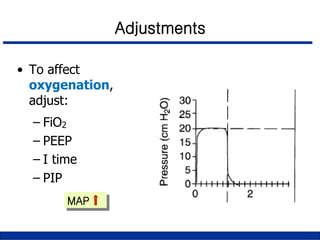
This document provides an overview of basic concepts and applications of mechanical ventilation. It discusses various ventilation modes including controlled, assisted, assist-control, IMV, and SIMV modes. It also covers settings such as tidal volume, respiratory rate, I:E ratio, and FIO2. Key aspects of setting up and monitoring mechanical ventilation are summarized, including how to initially set parameters based on patient size and desired minute ventilation. Factors that affect oxygenation and ventilation are outlined. Waveforms and pressure-volume loops are presented to illustrate lung mechanics under different conditions. The importance of monitoring airway pressures and compliance is emphasized to optimize ventilation.




















































































































![[03] 20200708 acid base](https://cdn.slidesharecdn.com/ss_thumbnails/0320200708acid-base-210114104354-thumbnail.jpg?width=640&height=640&fit=bounds)


