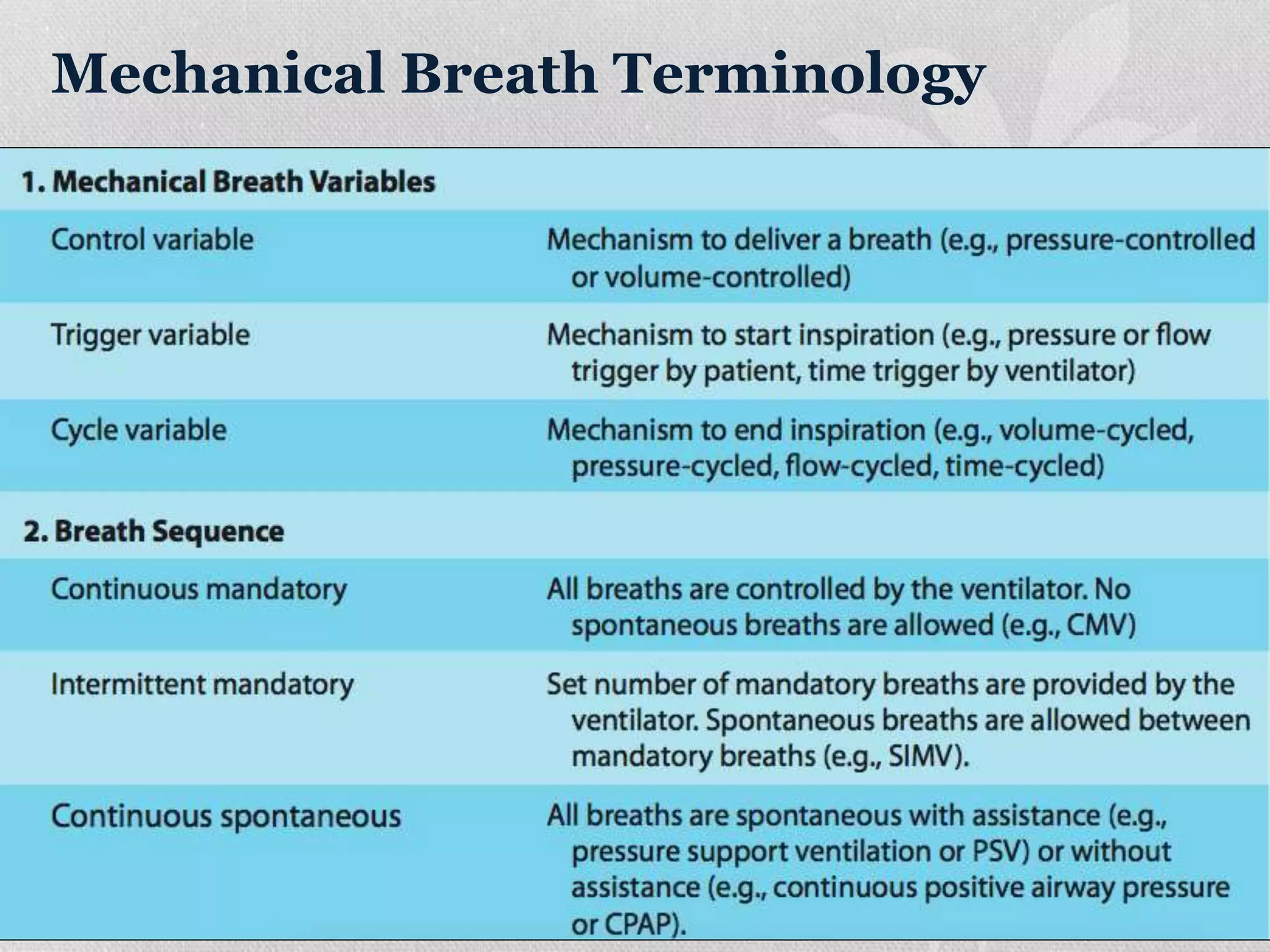
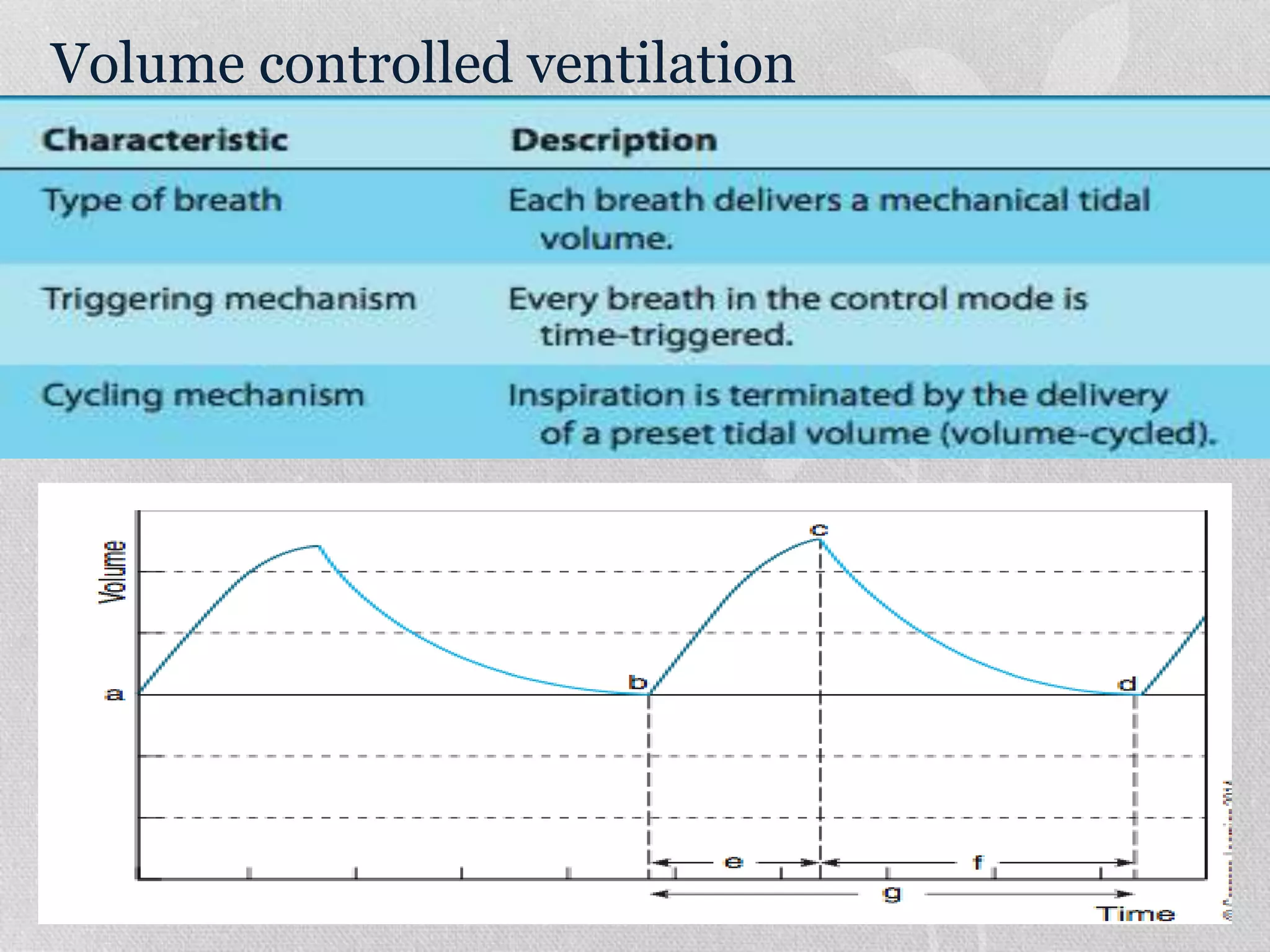
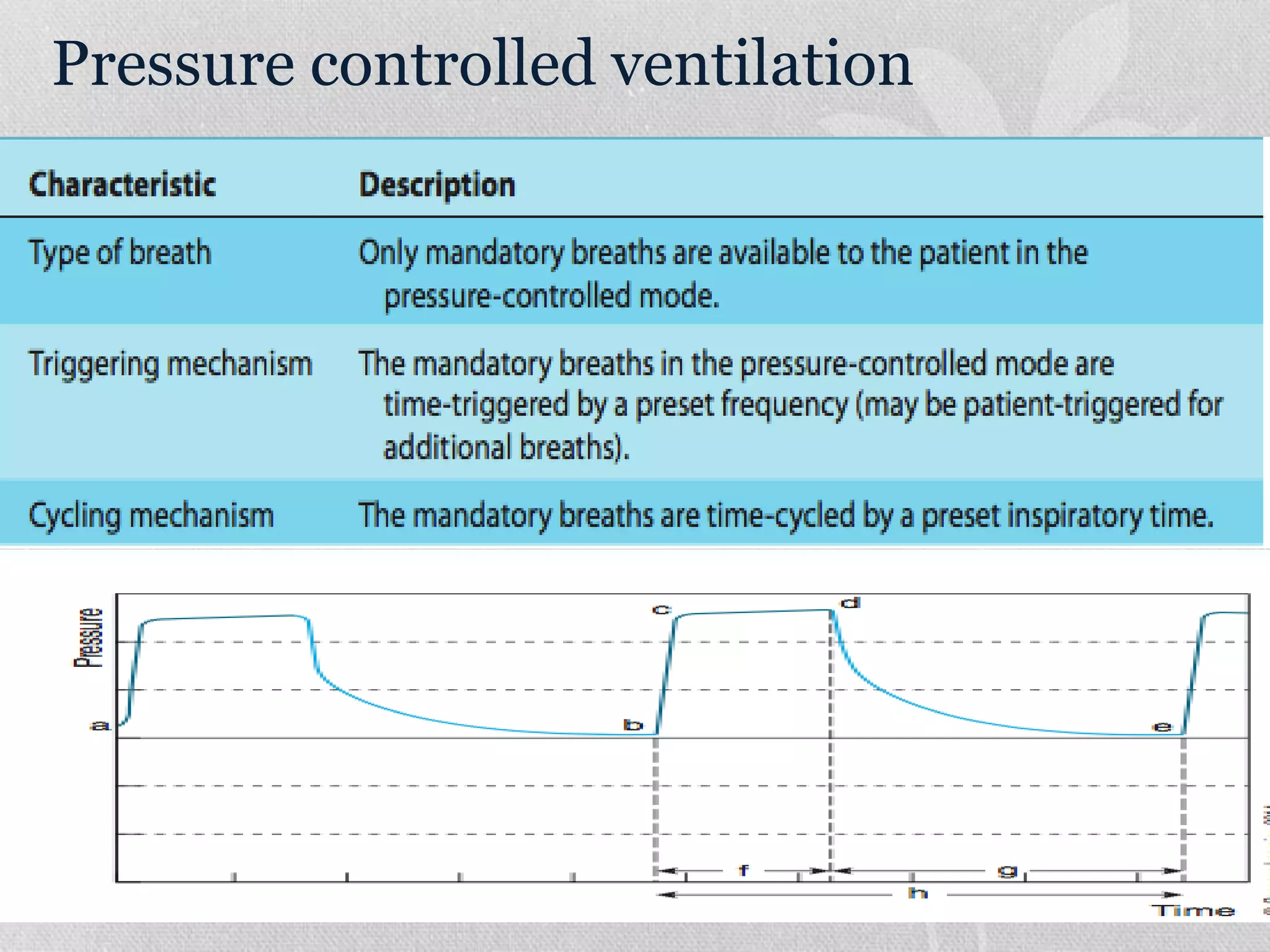
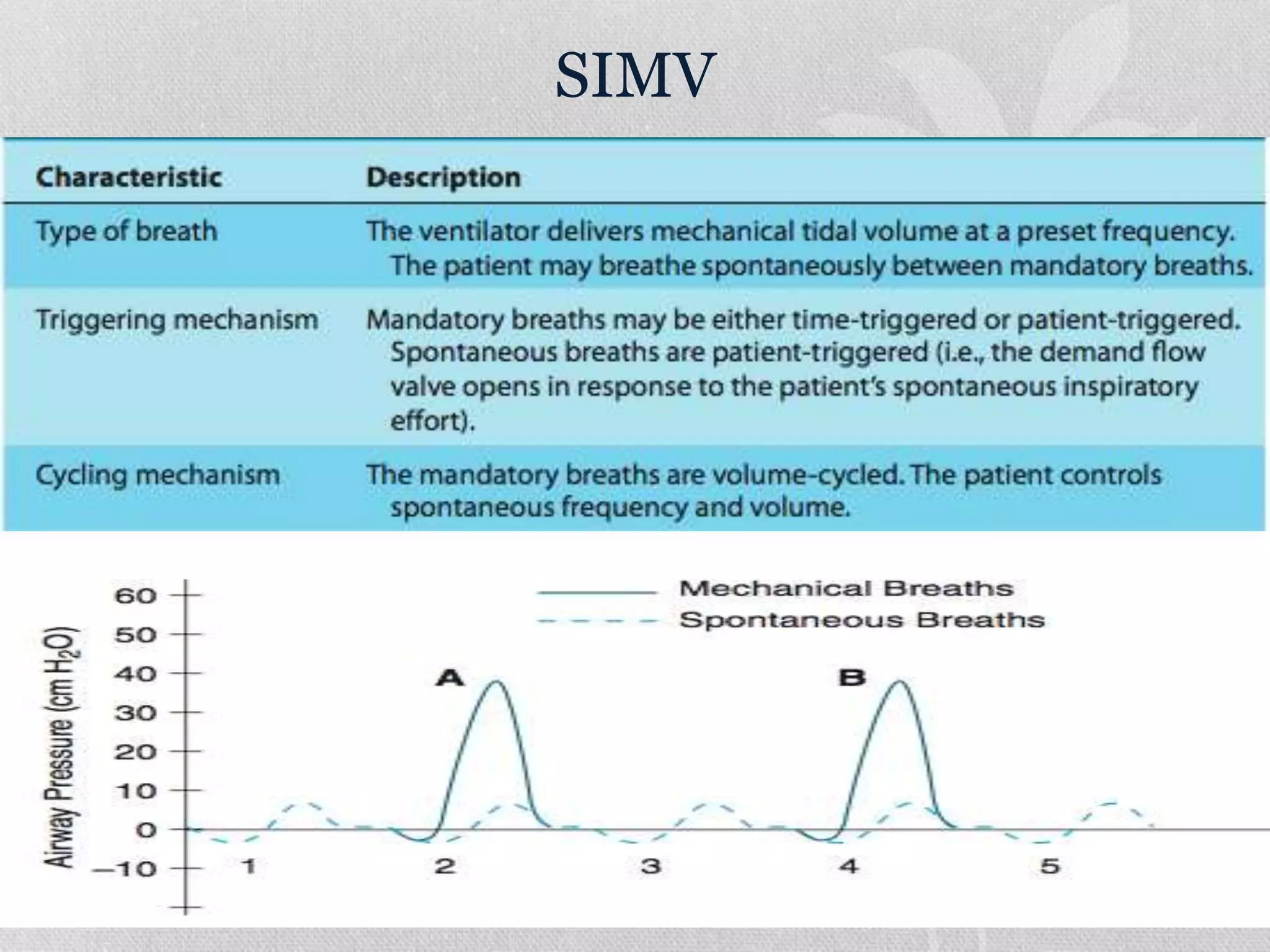
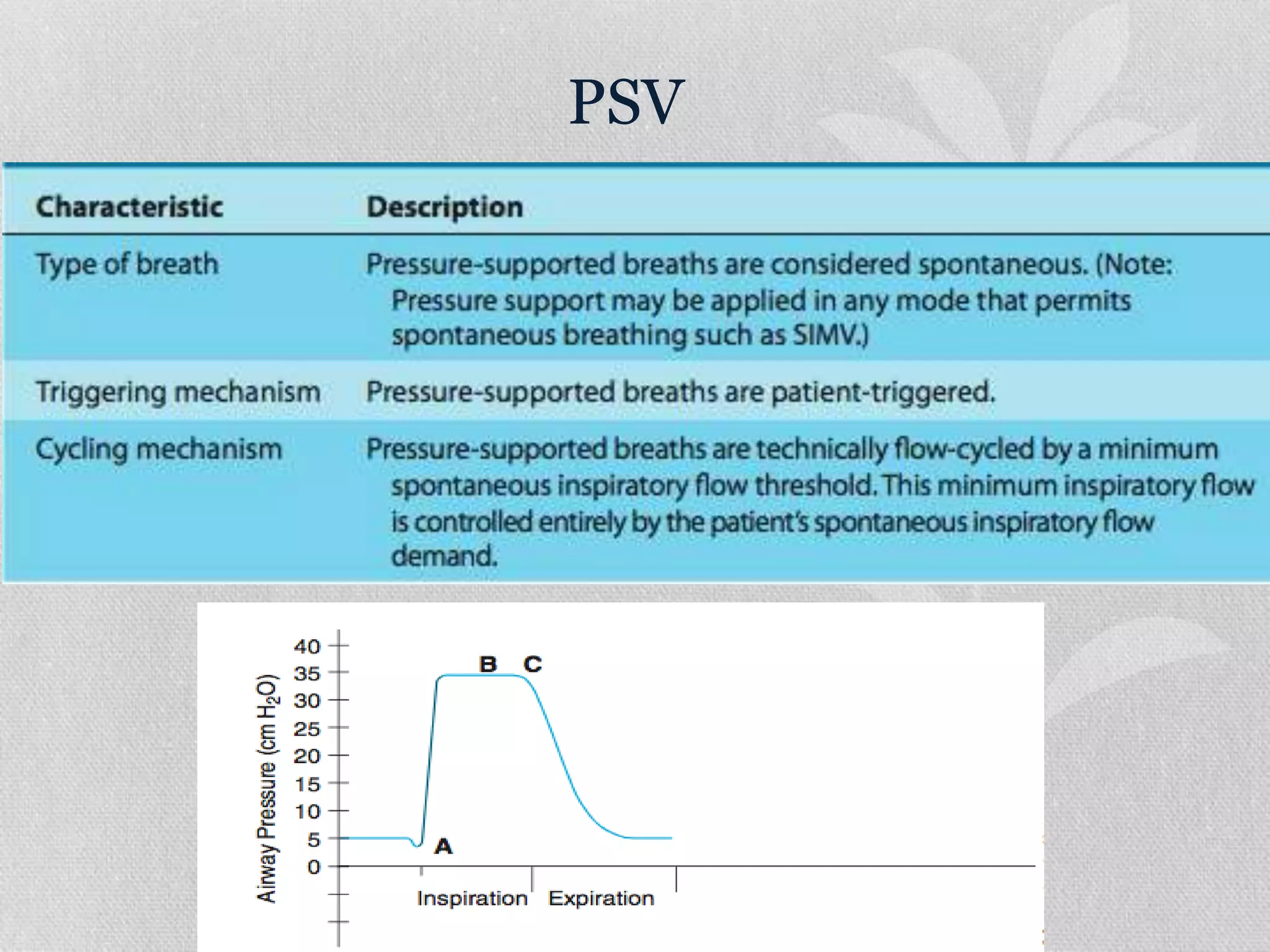
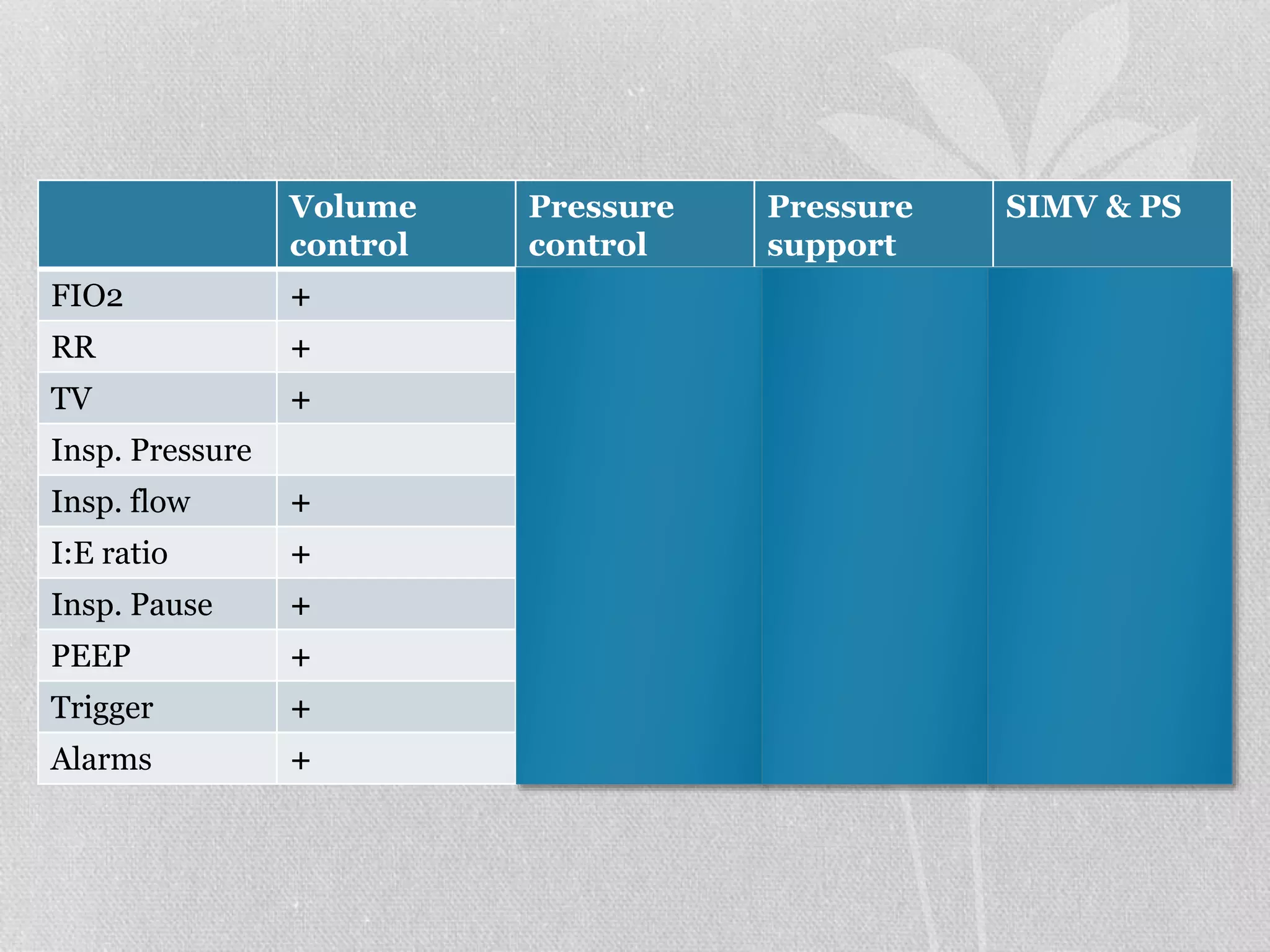
1. The document discusses various modes of mechanical ventilation including volume control, pressure control, SIMV, and PSV. It describes the settings, parameters, and considerations for each mode.
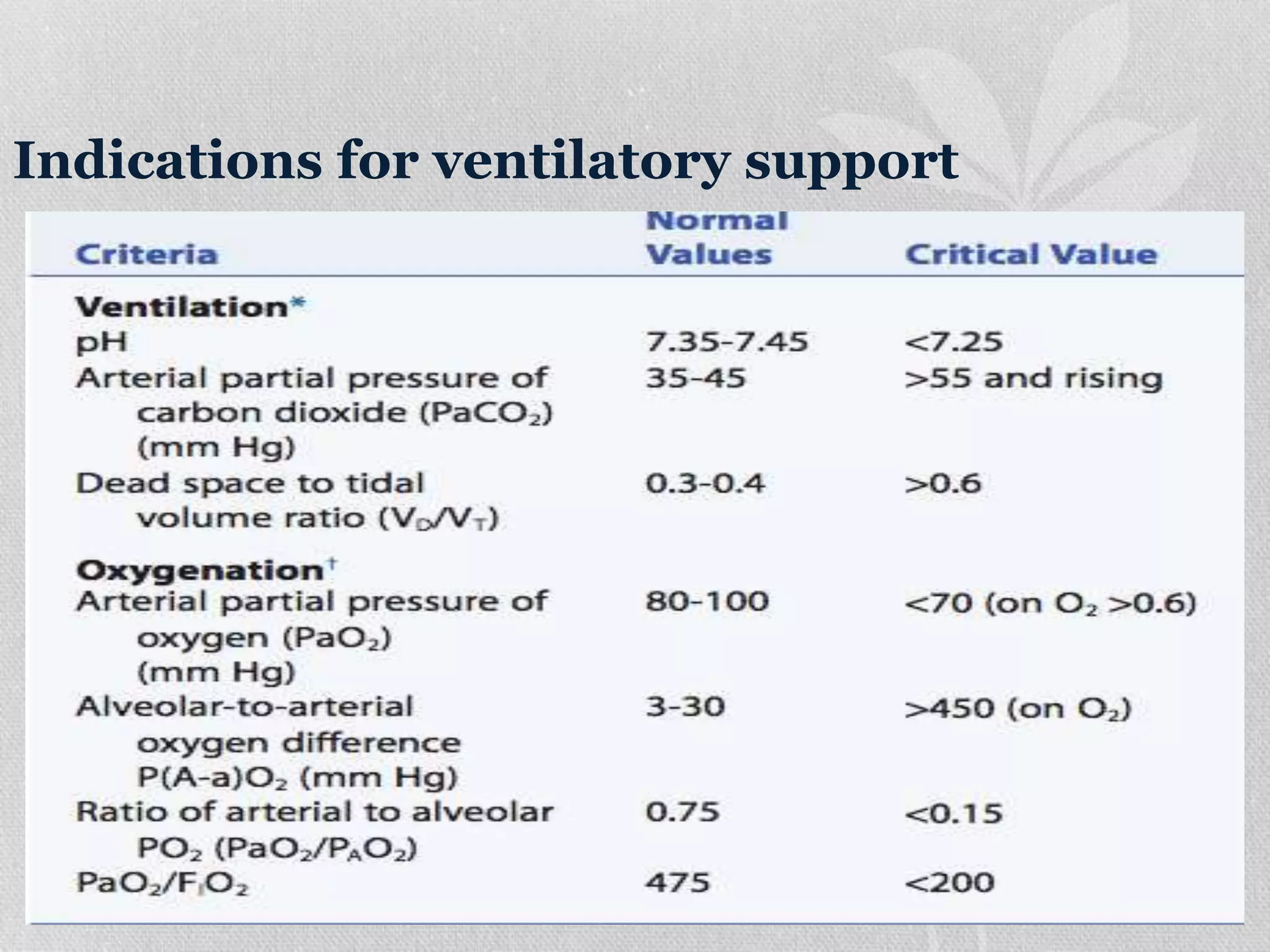
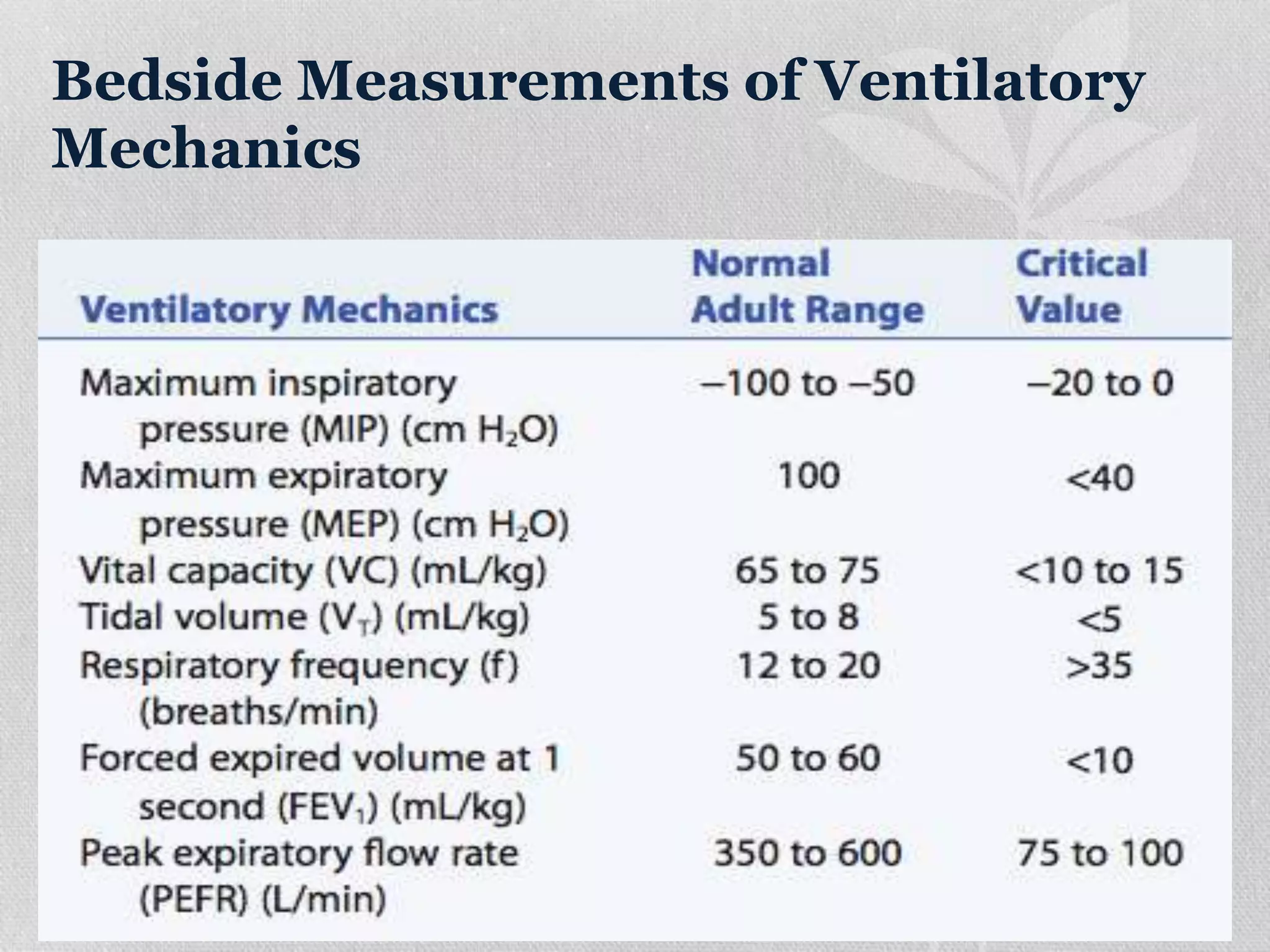
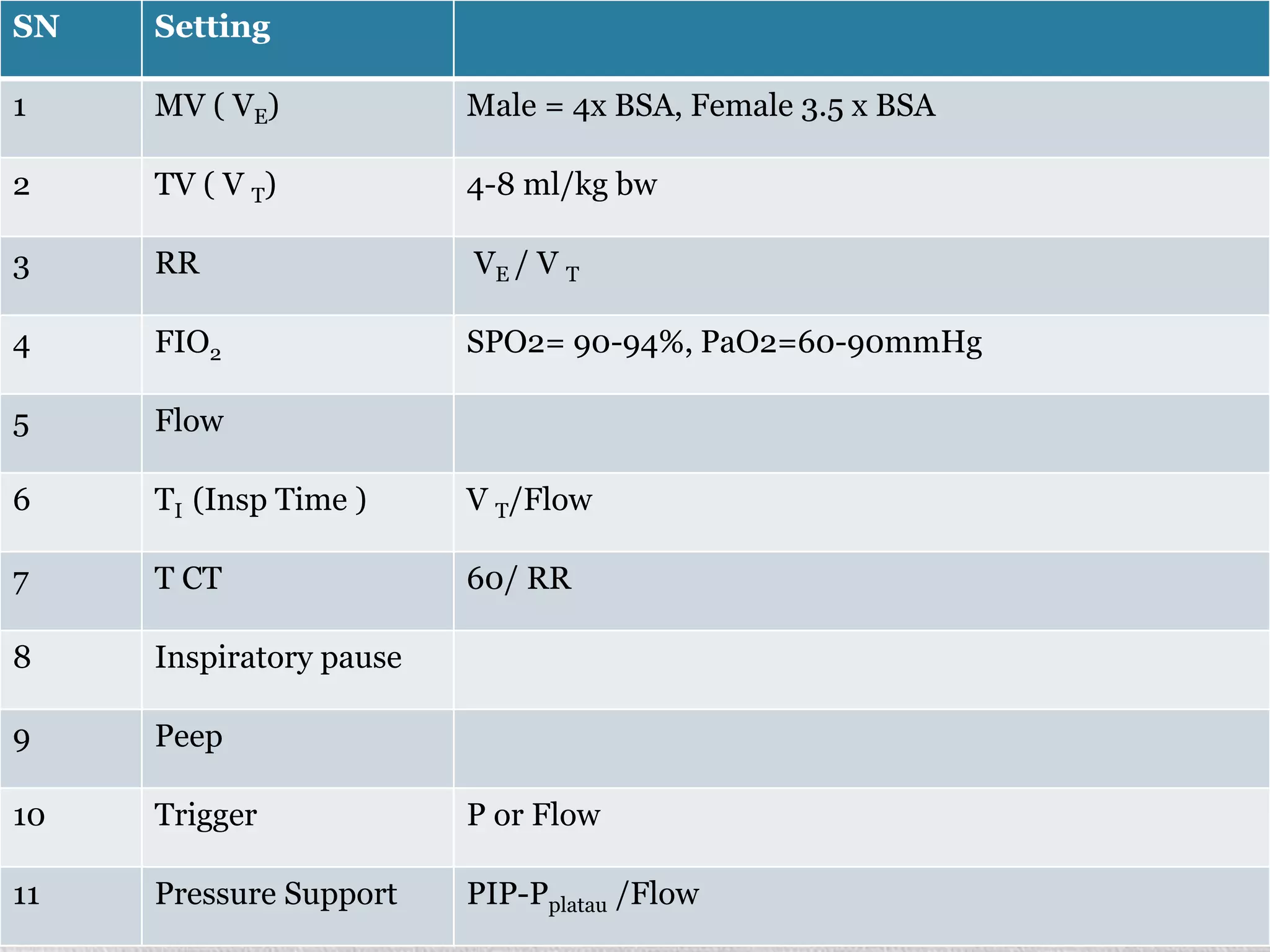
2. Initial ventilator settings should aim for adequate oxygenation and ventilation while minimizing work of breathing. Settings like tidal volume, respiratory rate, and PEEP are adjusted based on factors like patient size and condition.
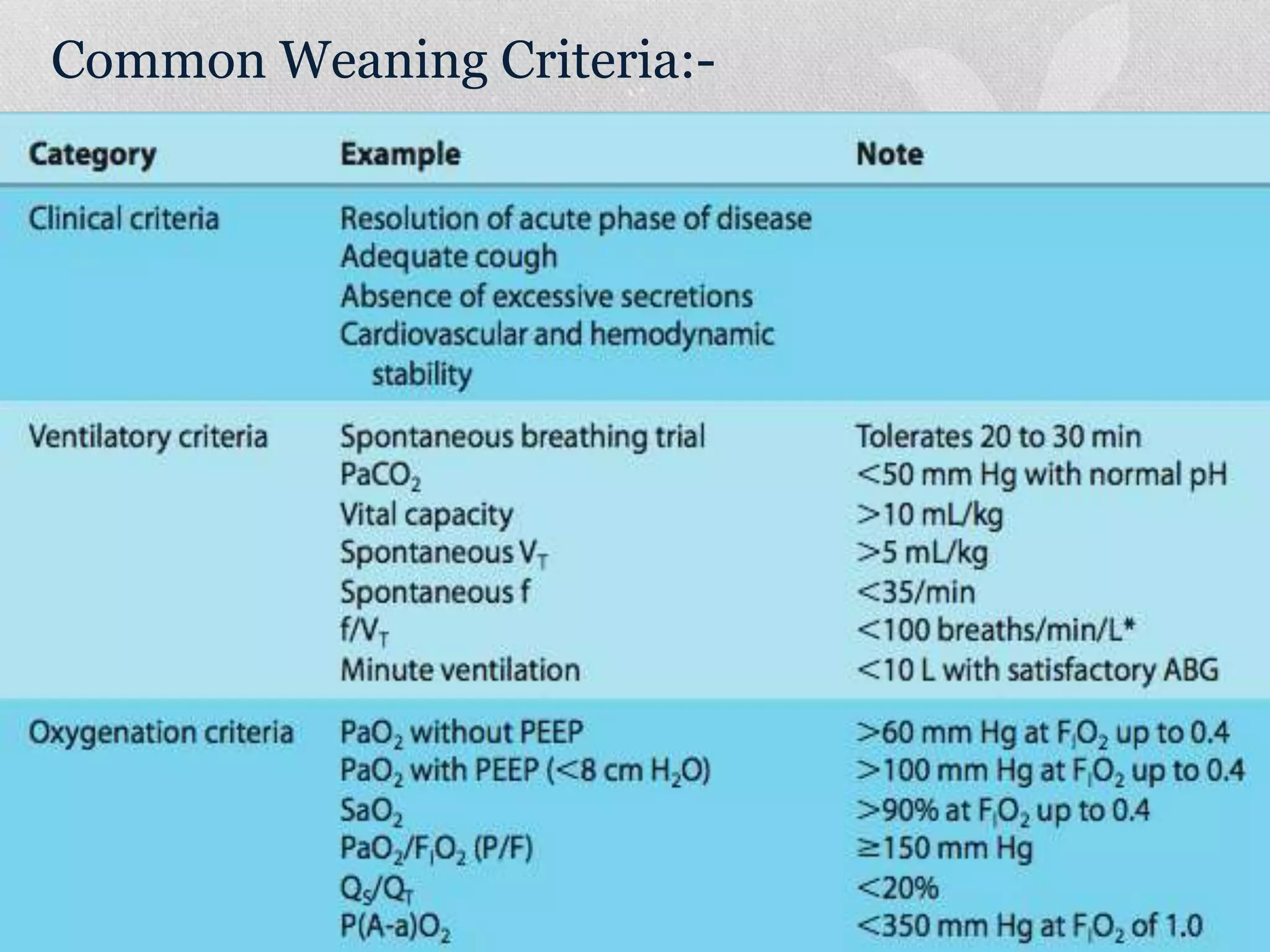
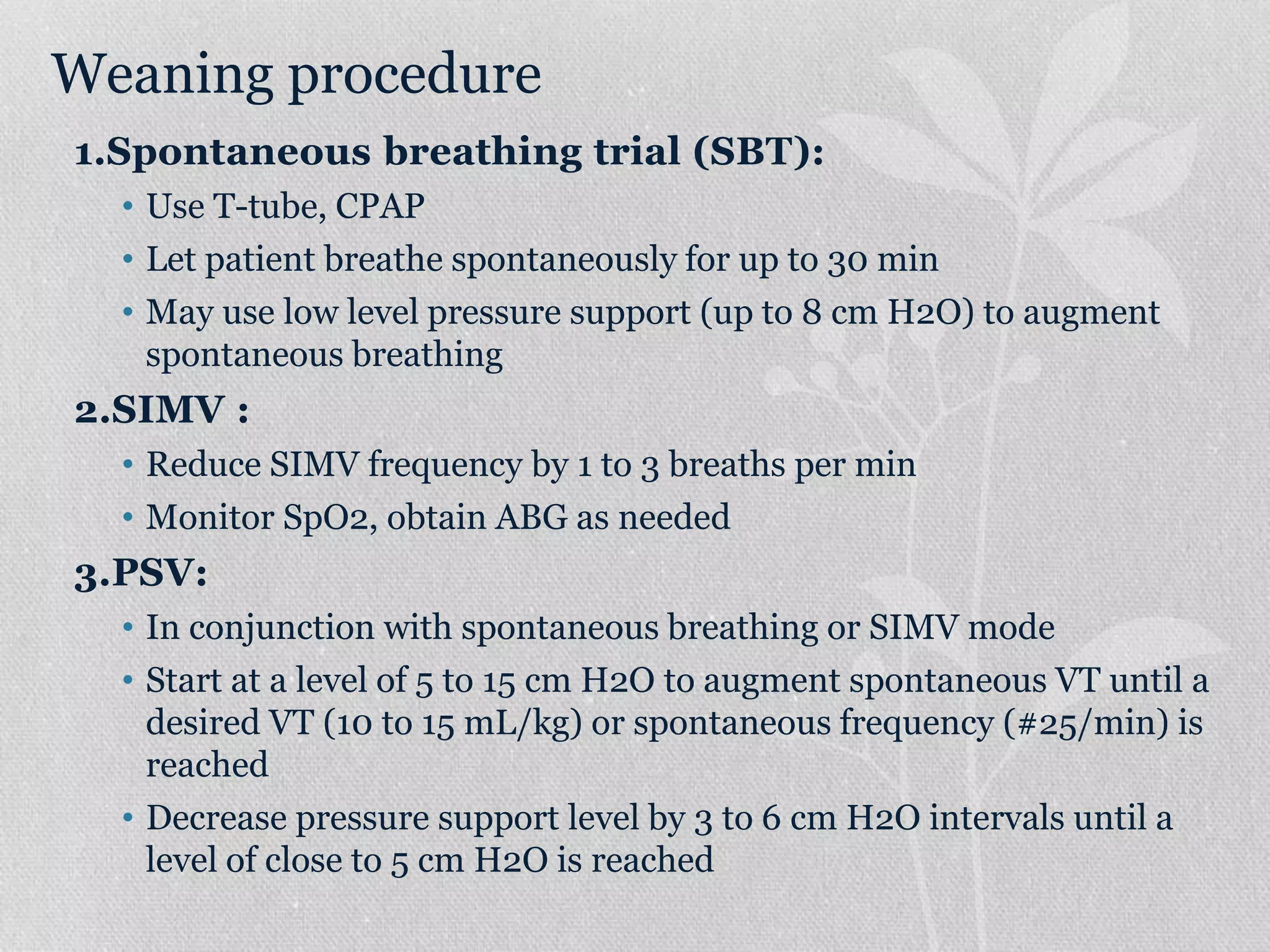
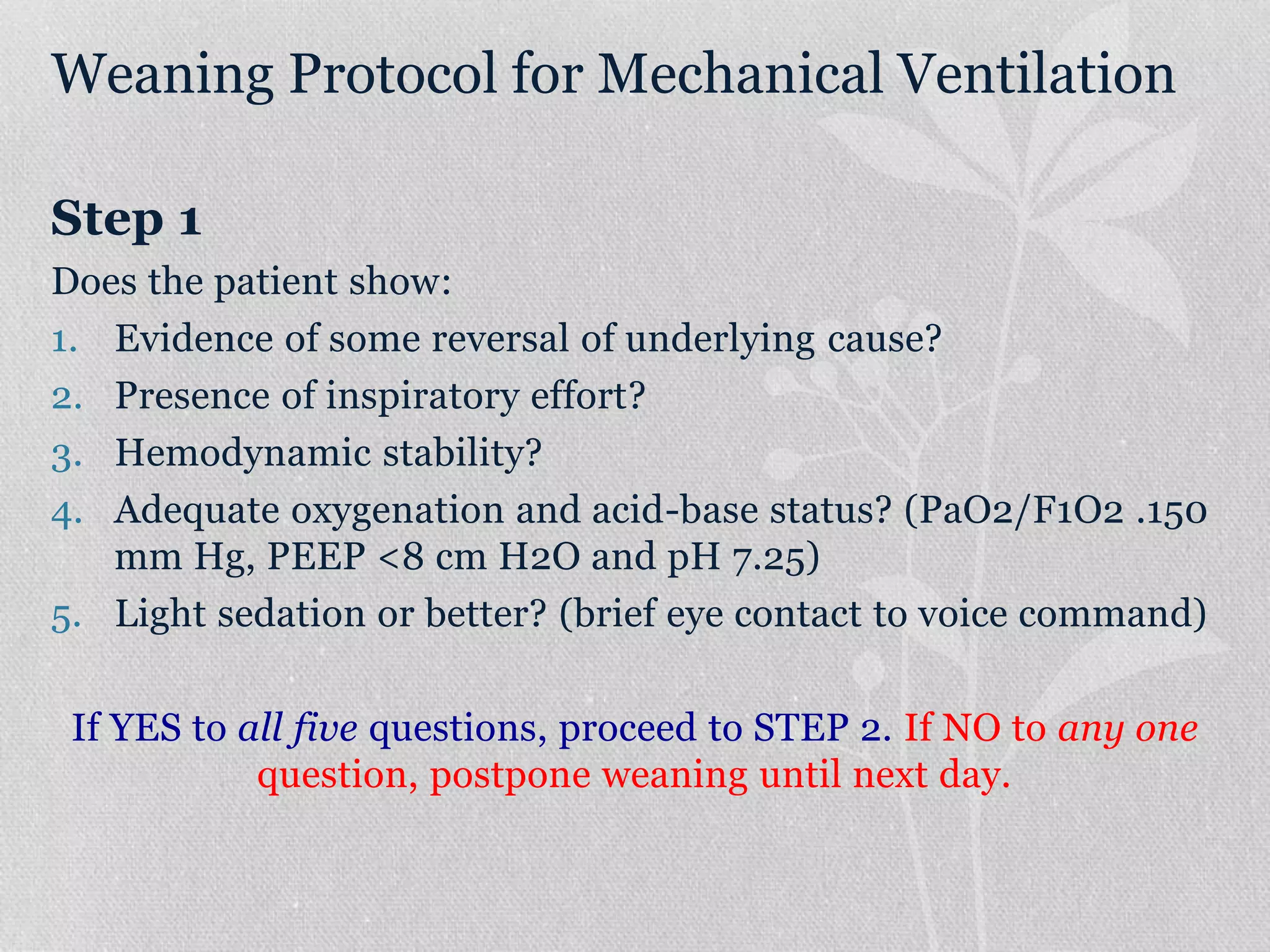
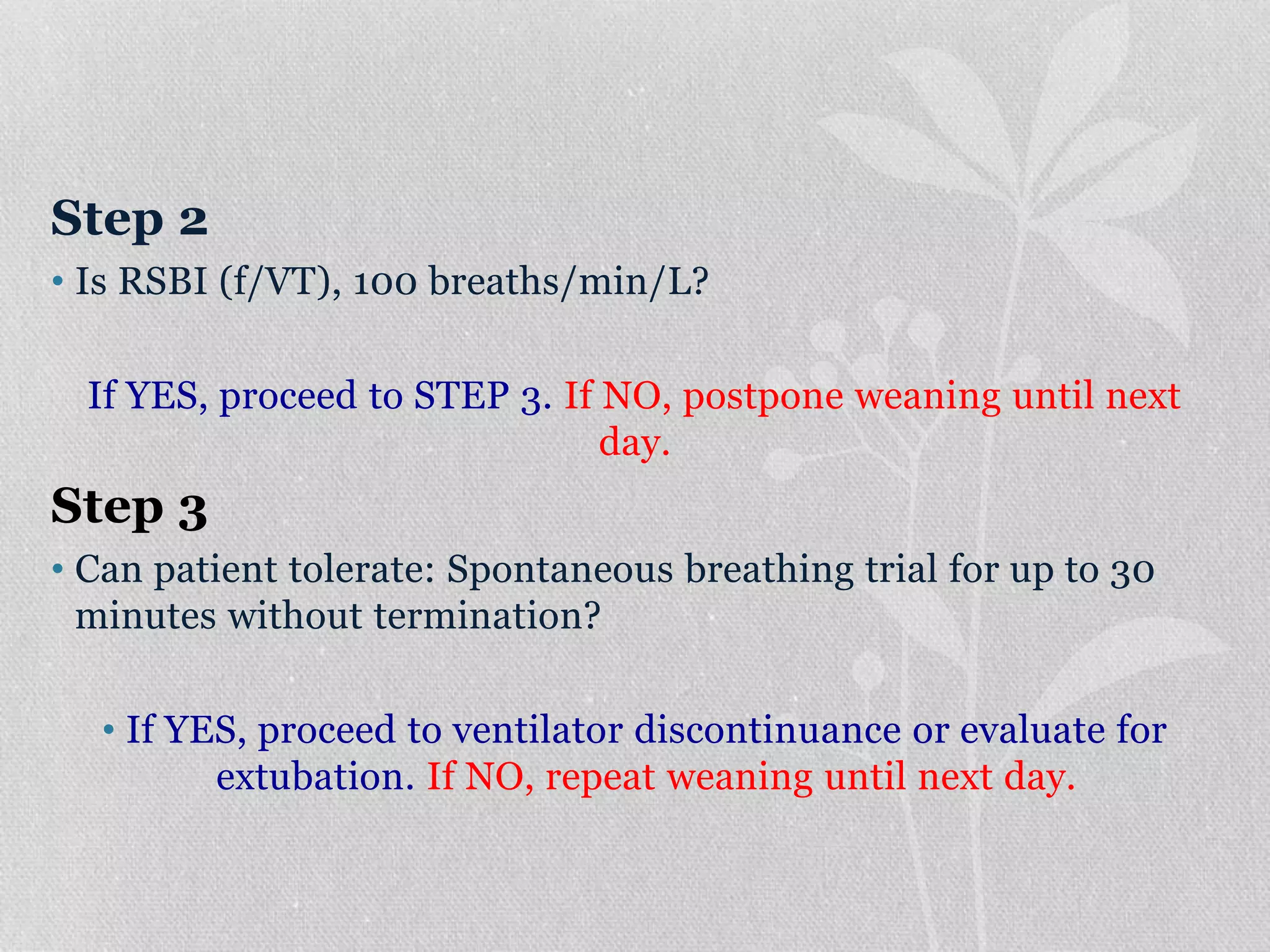
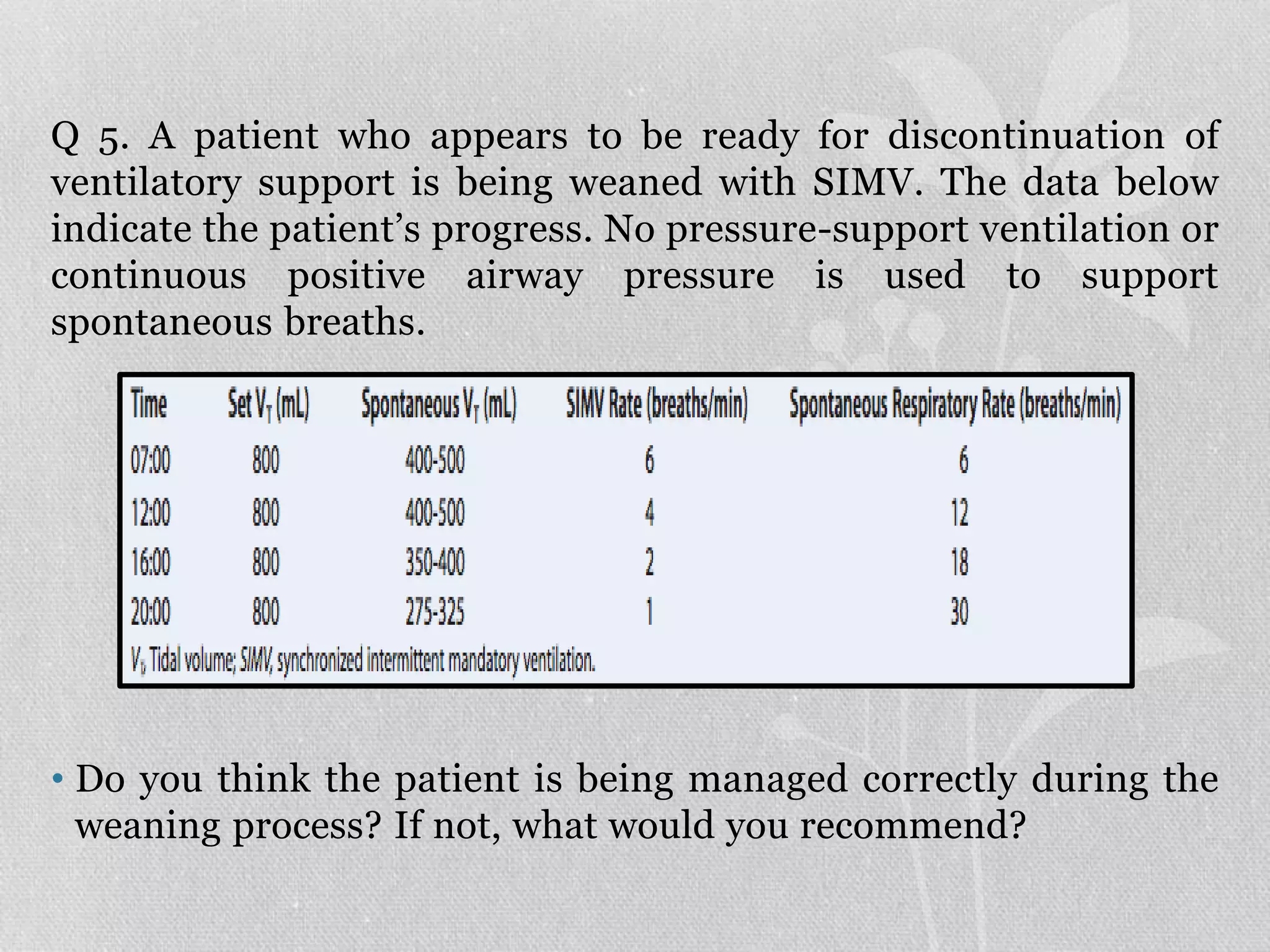
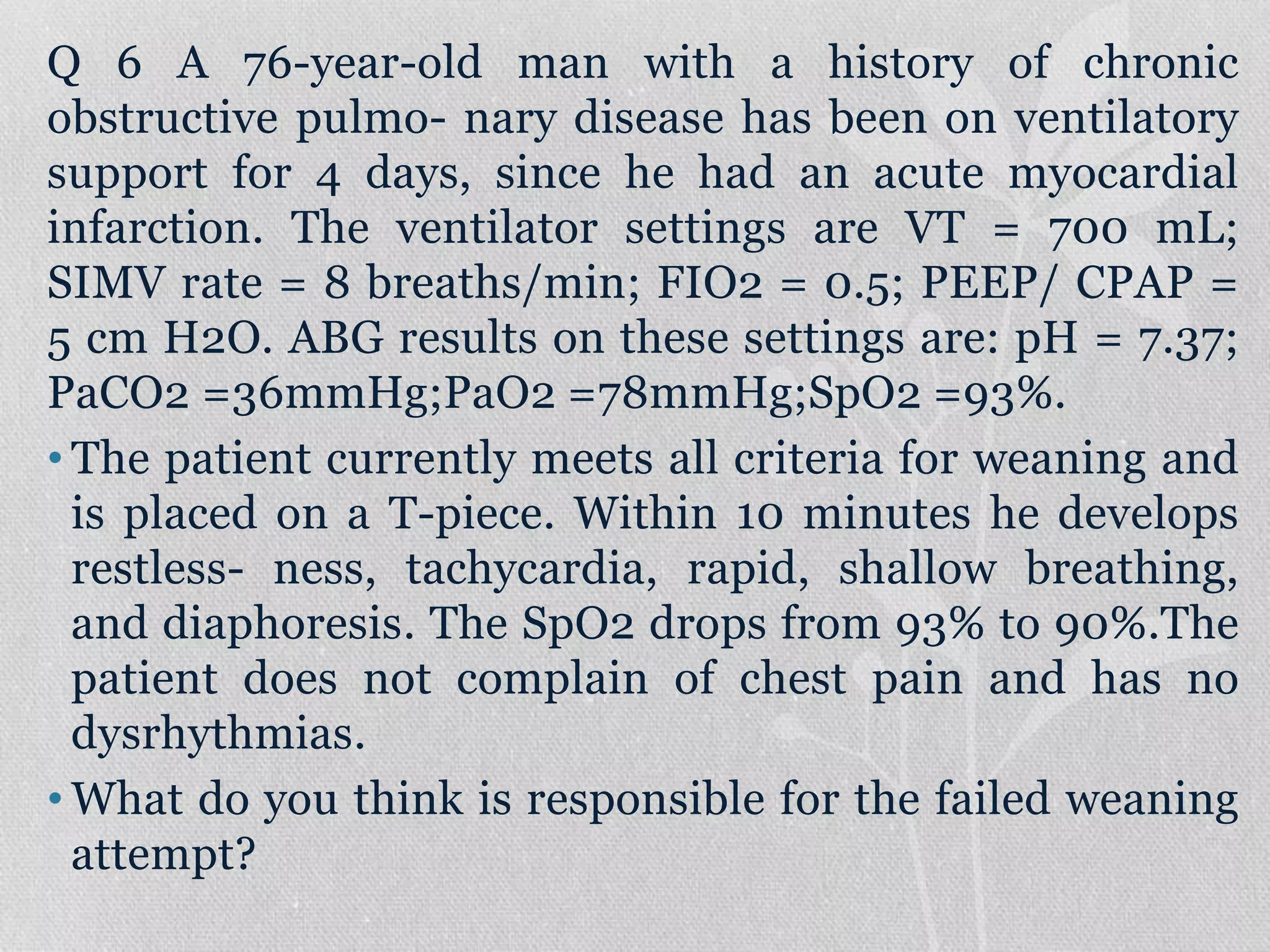
3. Weaning from mechanical ventilation involves gradually reducing support through methods like spontaneous breathing trials, decreasing SIMV frequency, and lowering pressure support levels to assess the patient's ability to breathe independently. Readiness criteria and a stepwise protocol are