Downloaded 1,348 times
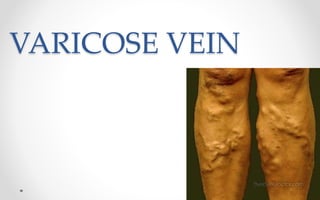

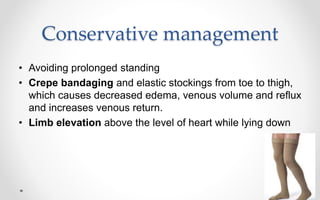
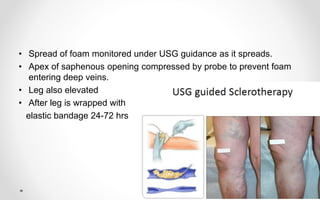



Varicose veins are dilated, elongated superficial veins caused by venous hypertension. They most commonly occur in males in India and affect the left lower limb. The superficial venous system can become incompetent due to family history, pregnancy, aging, deep vein thrombosis, oral contraceptives or obesity. Treatment options include compression stockings and bandages, sclerotherapy using chemicals to obliterate veins, and high ligation and stripping surgery to remove veins. Nursing care focuses on leg elevation, walking exercises, and wearing compression stockings after treatment.





































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)

















