Downloaded 528 times
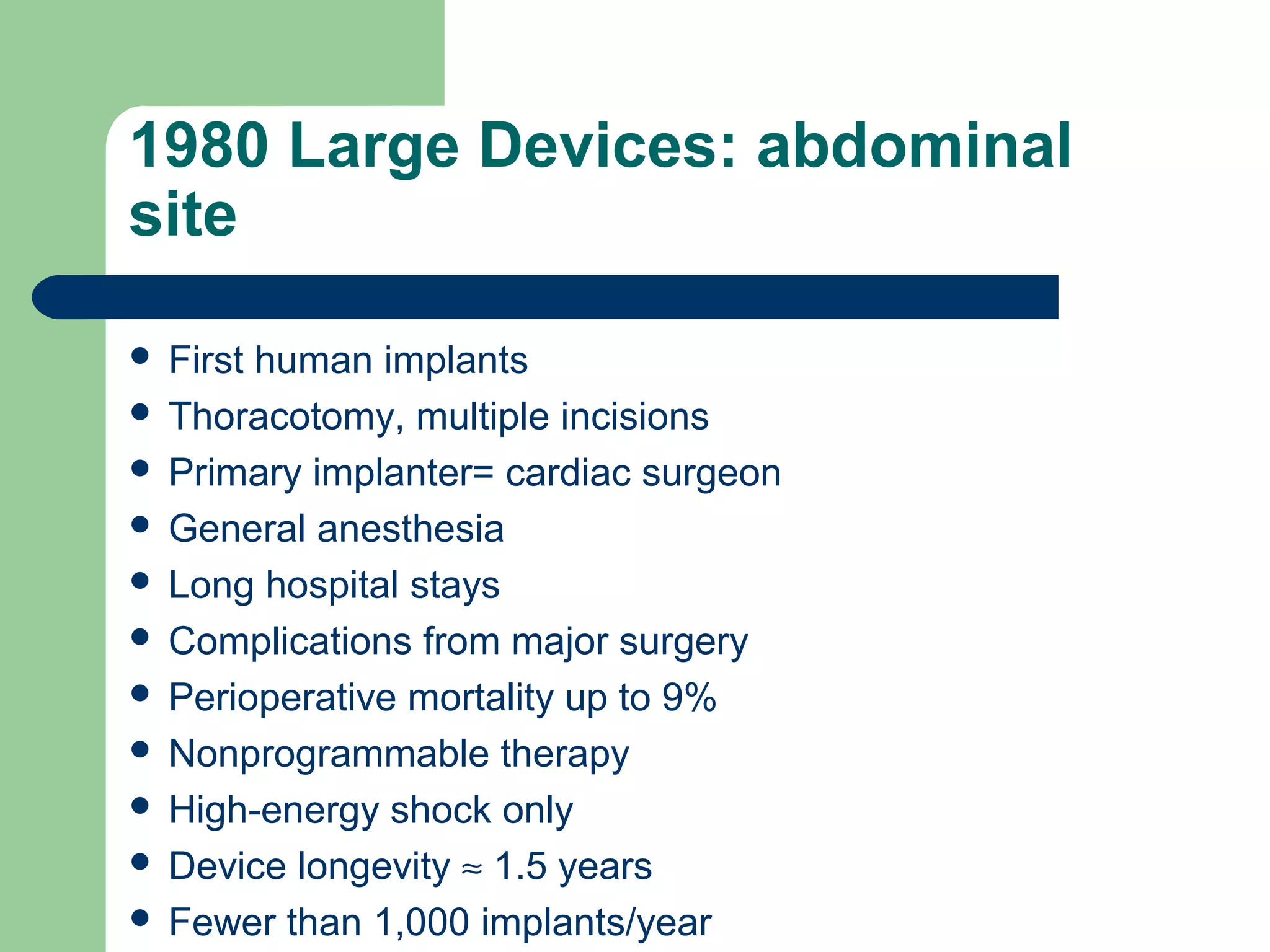
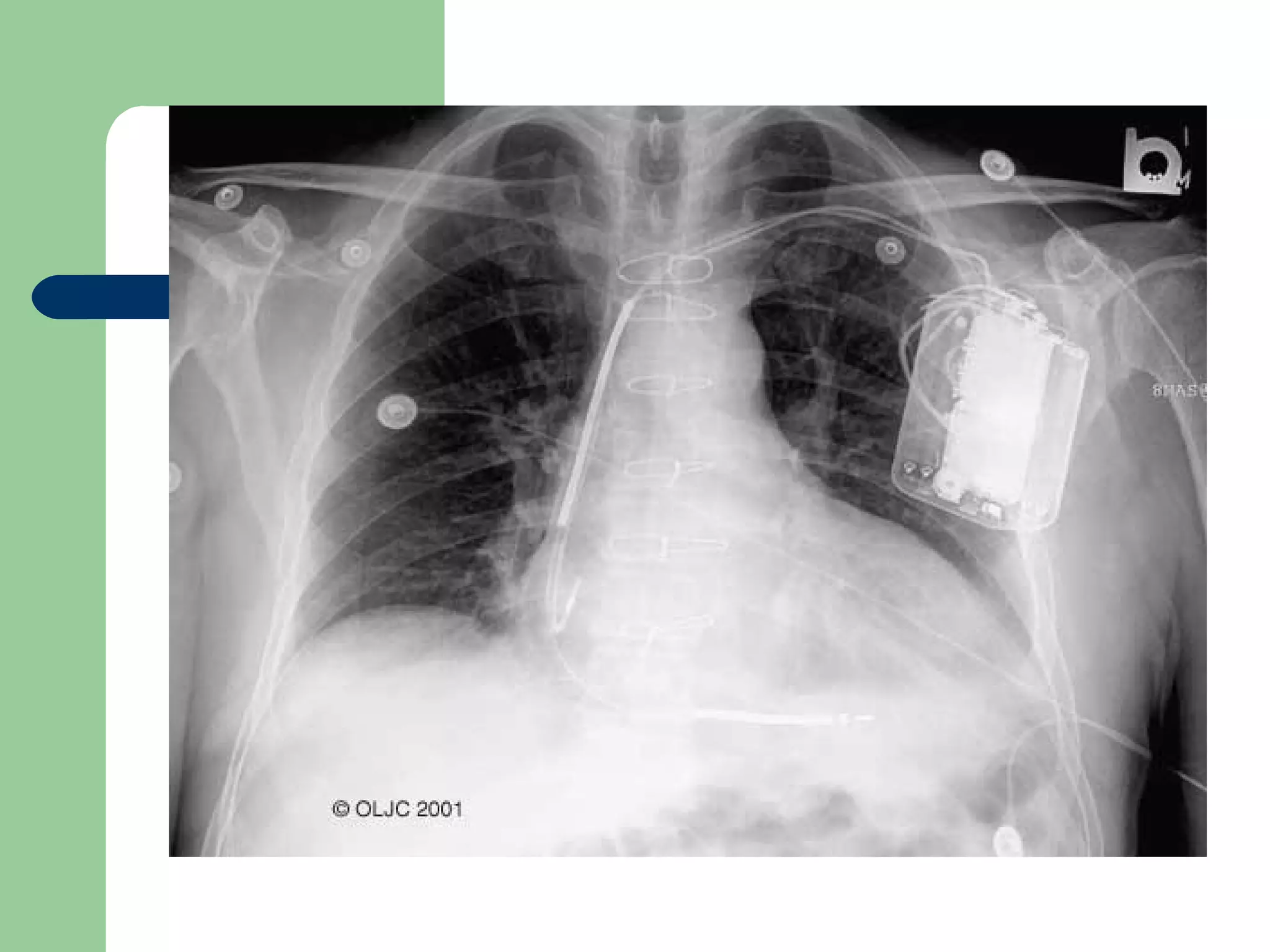
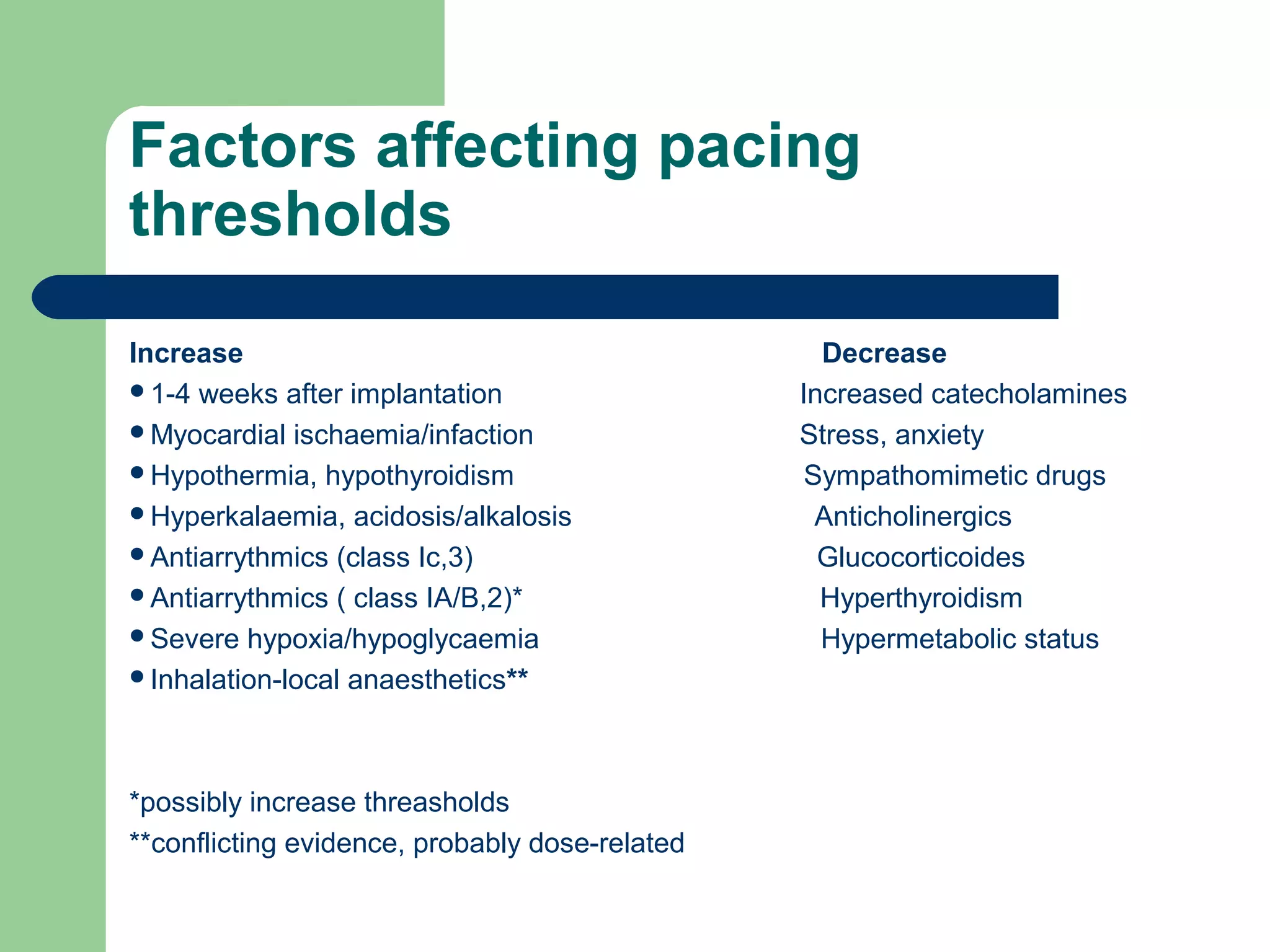










This document discusses pacemakers and their implications for anesthesia. It provides a brief history of pacemaker development from large abdominal devices in 1980 to today's small pectoral devices. It covers pacemaker indications, types of pacing modes, factors affecting pacing thresholds, preoperative evaluation, intraoperative management considerations, and the effect of magnet application. Pacemaker dependent patients require ECG monitoring and backup pacing during anesthesia given risks of electromagnetic interference or inappropriate pacing inhibition or triggering.





















![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)













































