Downloaded 591 times
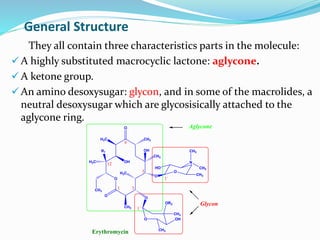

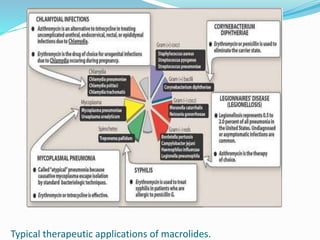
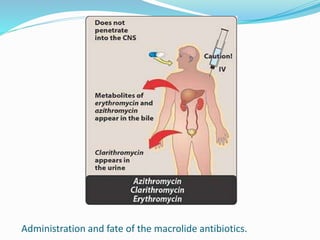
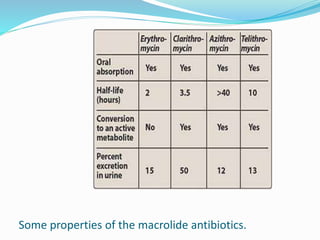
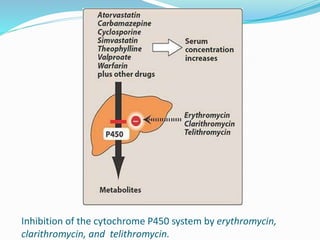

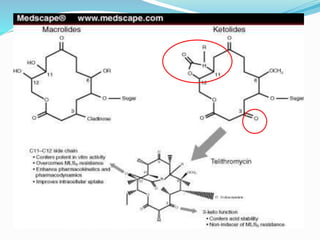
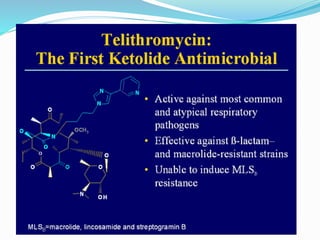

This document provides an overview of macrolide antibiotics. It discusses their history, chemical structure, classification, mechanisms of action, spectrum of activity, resistance, pharmacokinetics, adverse effects and clinical applications. Macrolides are a class of antibiotics that work by inhibiting bacterial protein synthesis. They are effective against many gram-positive and some gram-negative bacteria. Common macrolides discussed include erythromycin, clarithromycin, azithromycin and ketolides like telithromycin.























































































