Downloaded 10 times

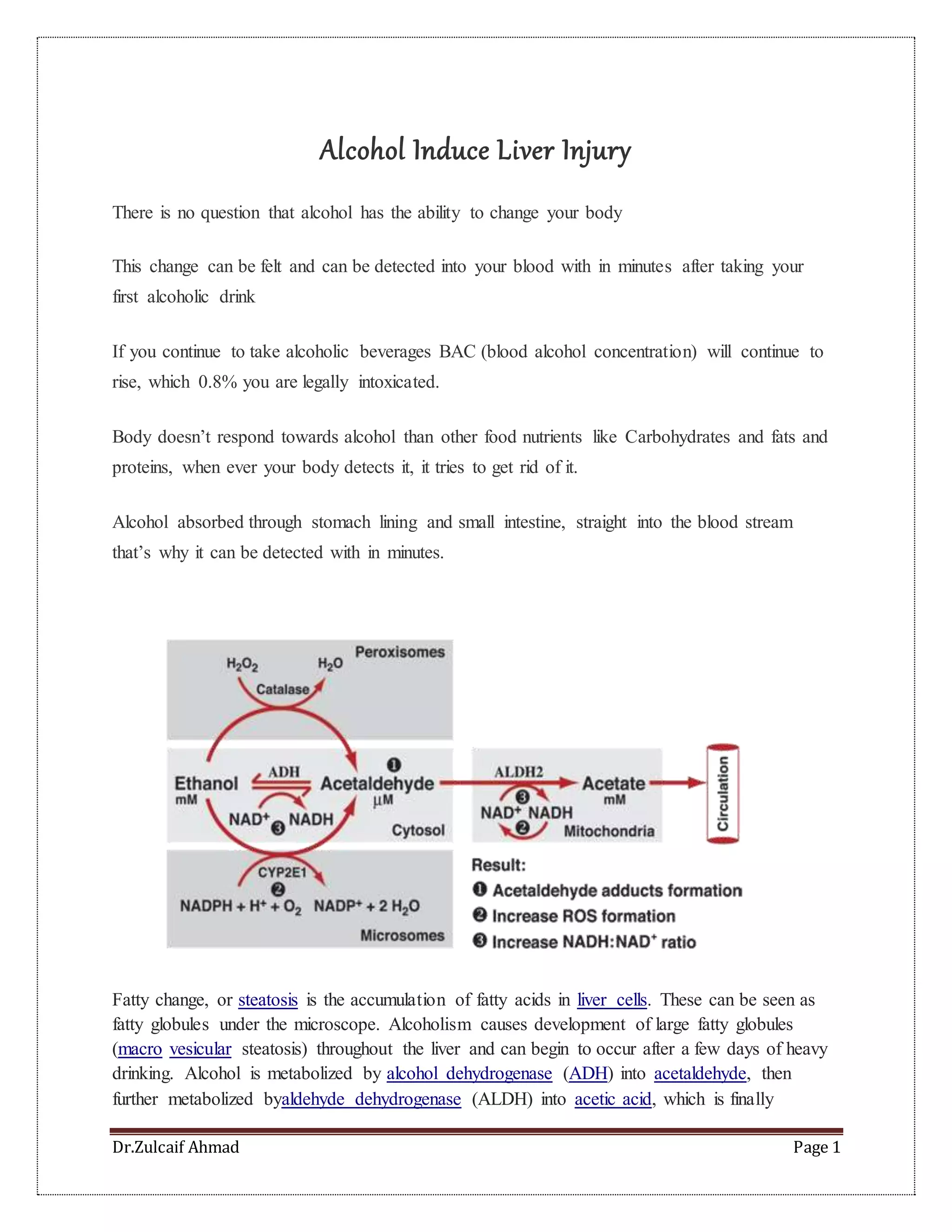





This document summarizes the effects of alcohol on the liver, including fatty liver, alcoholic hepatitis, and cirrhosis. It discusses how alcohol is metabolized and causes a buildup of fatty acids in the liver over time with heavy drinking. Inflammation occurs which can progress to fibrosis and scarring of the liver. Symptoms range from jaundice to liver failure. Diagnosis involves physical examination. Treatment focuses on supportive care, with controversies around corticosteroids and trials of other medications to reduce inflammation. Severe cases may require liver transplantation.























































![Alcoholic liver disease [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/alcoholicliverdiseaseautosaved-210106093112-thumbnail.jpg?width=640&height=640&fit=bounds)


















































