Downloaded 267 times
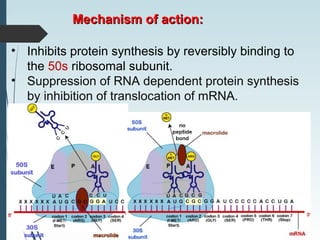


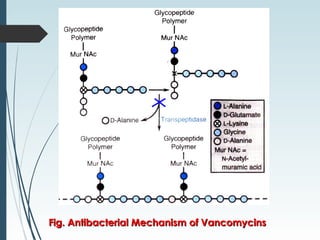


1) Macrolides, lincosamides, and glycopeptides are classes of antimicrobials. Macrolides like erythromycin and azithromycin are bacteriostatic and act by inhibiting bacterial protein synthesis. Lincosamides like clindamycin have similar properties. Glycopeptides like vancomycin and teicoplanin are bactericidal against gram-positive cocci including MRSA. 2) These drugs are used to treat respiratory, skin and soft tissue infections caused by susceptible bacteria. However, they can cause adverse effects like diarrhea, liver toxicity, and ototoxicity. Resistance occurs through modifications of the bacterial ribosome or cell membrane. 3) Proper























































































