Downloaded 437 times
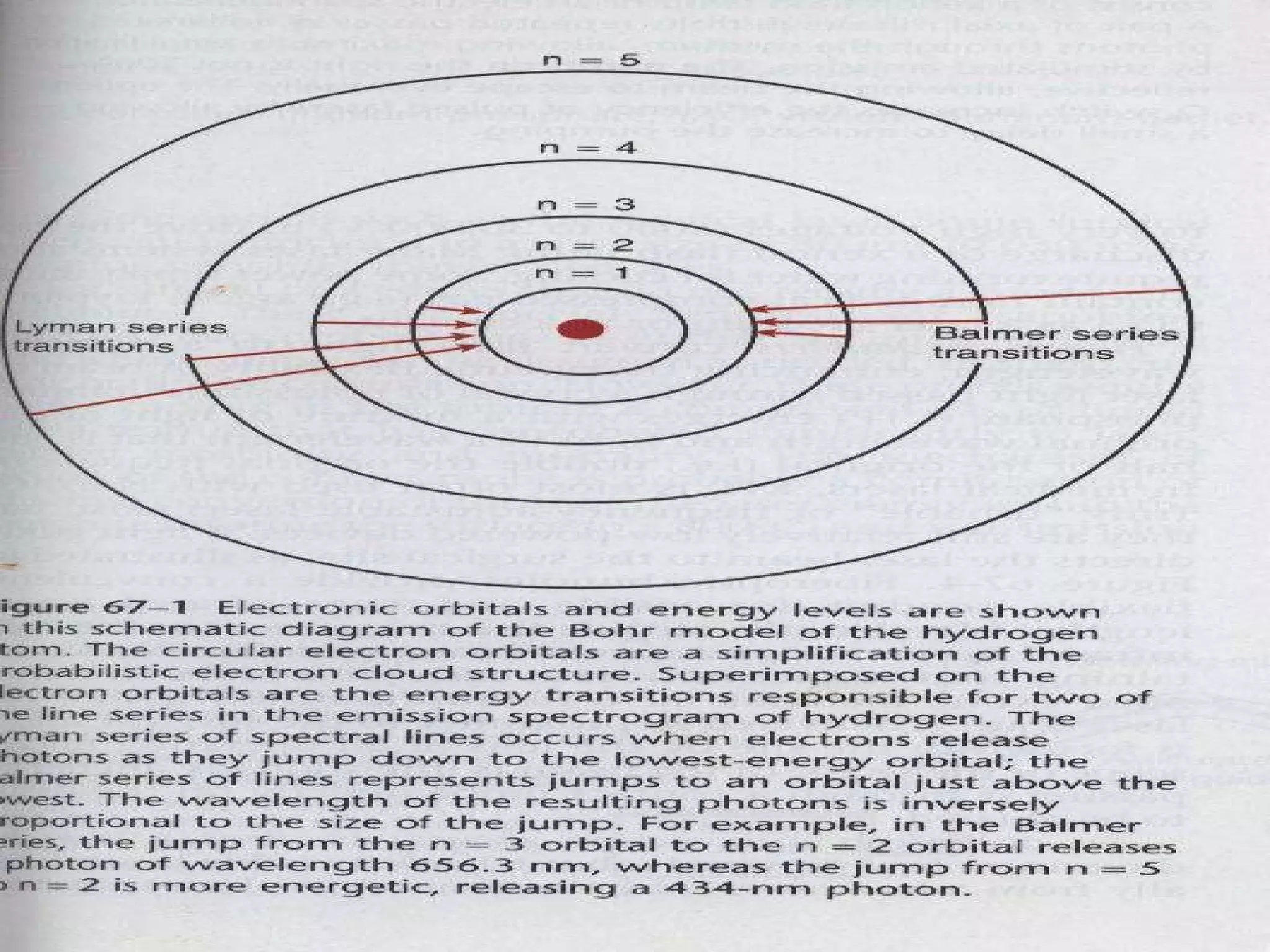
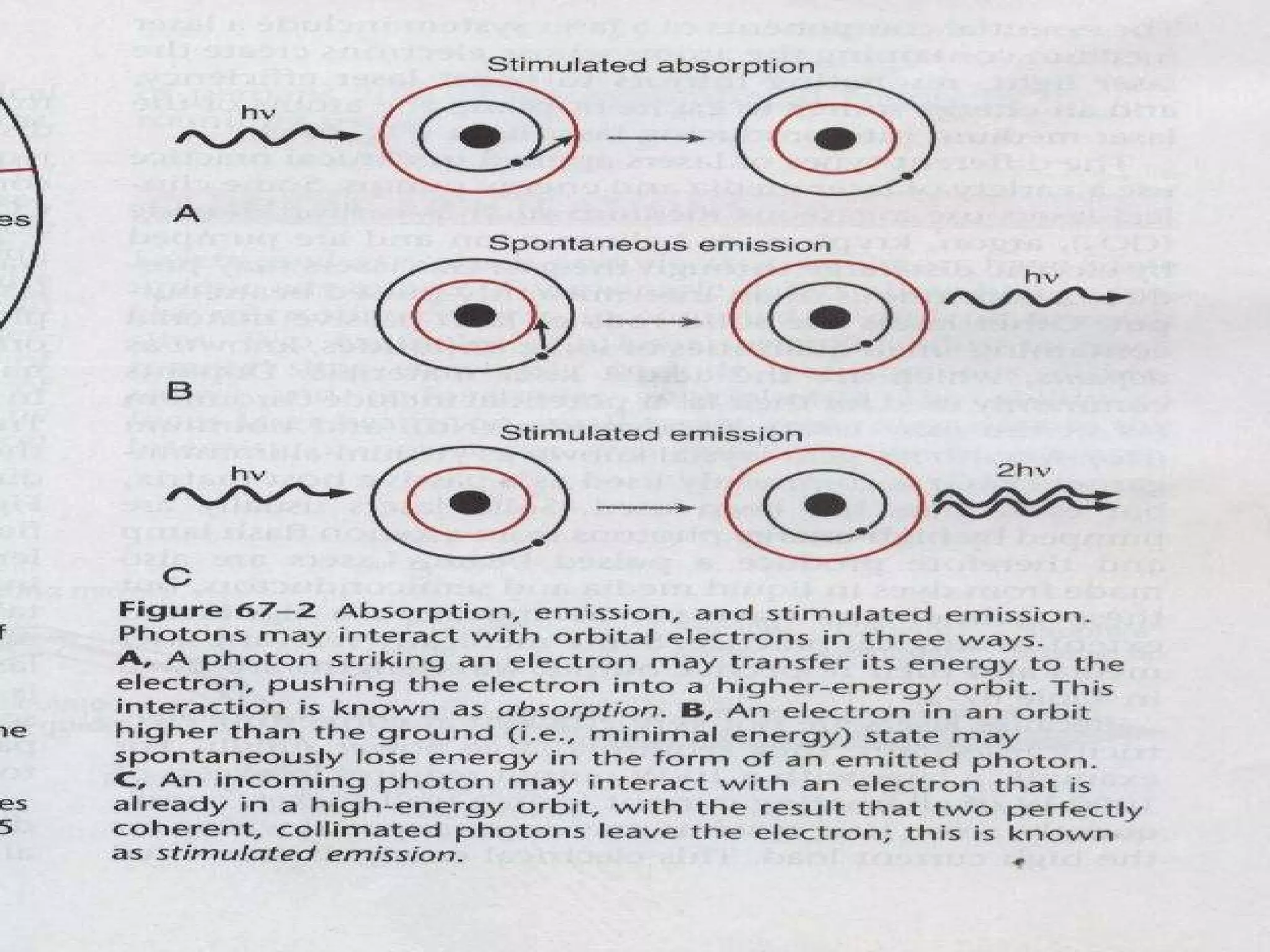
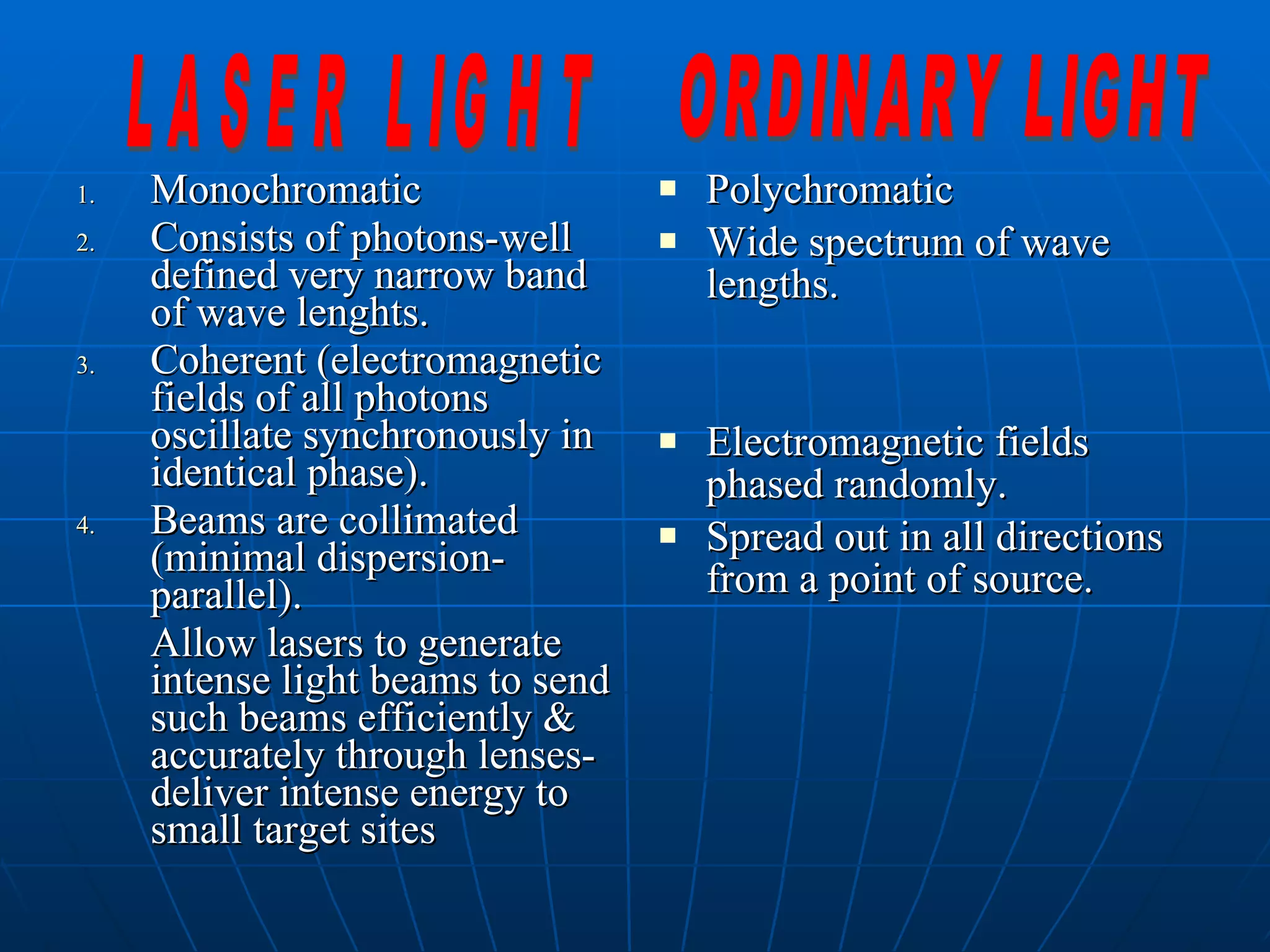

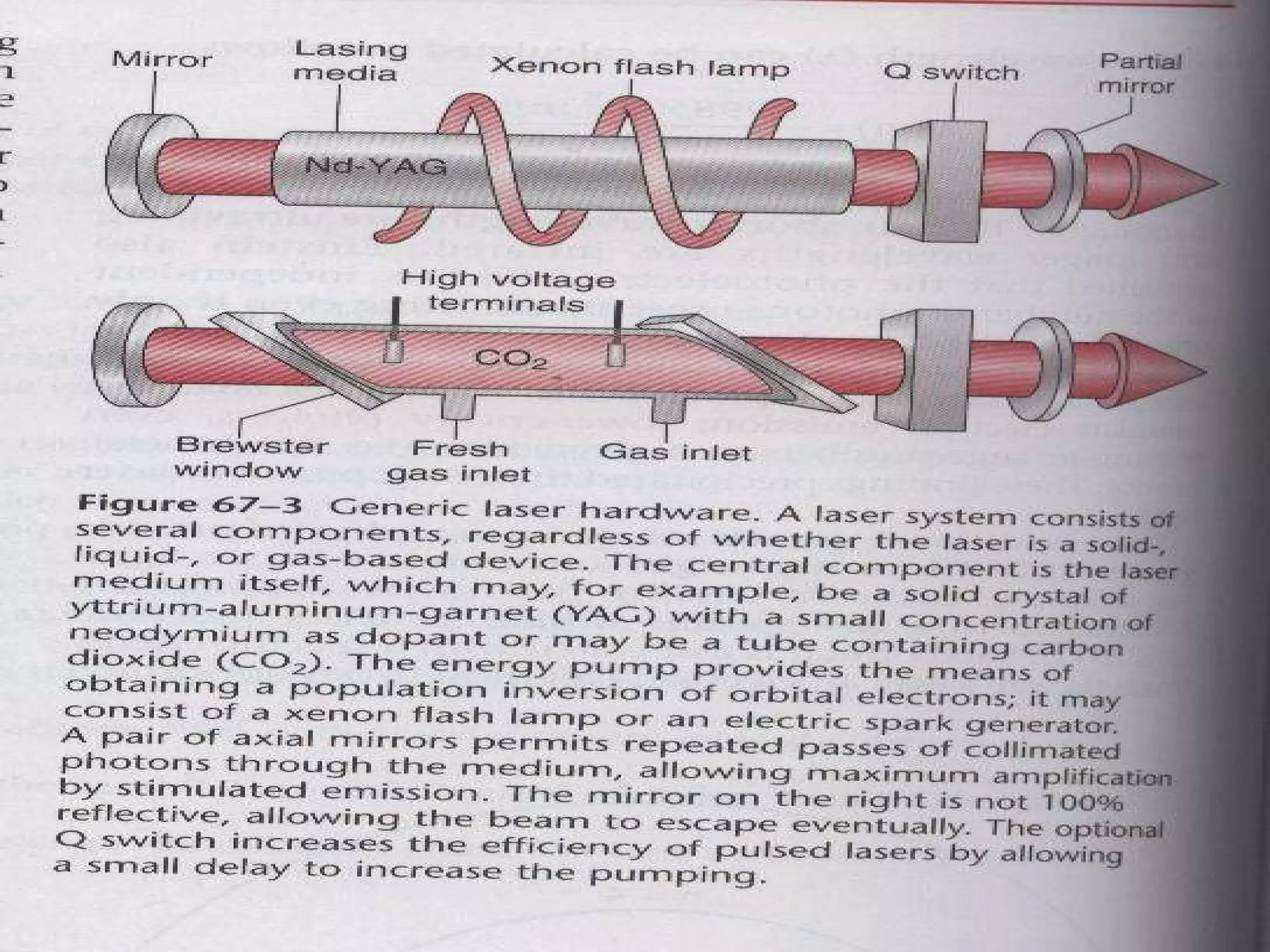
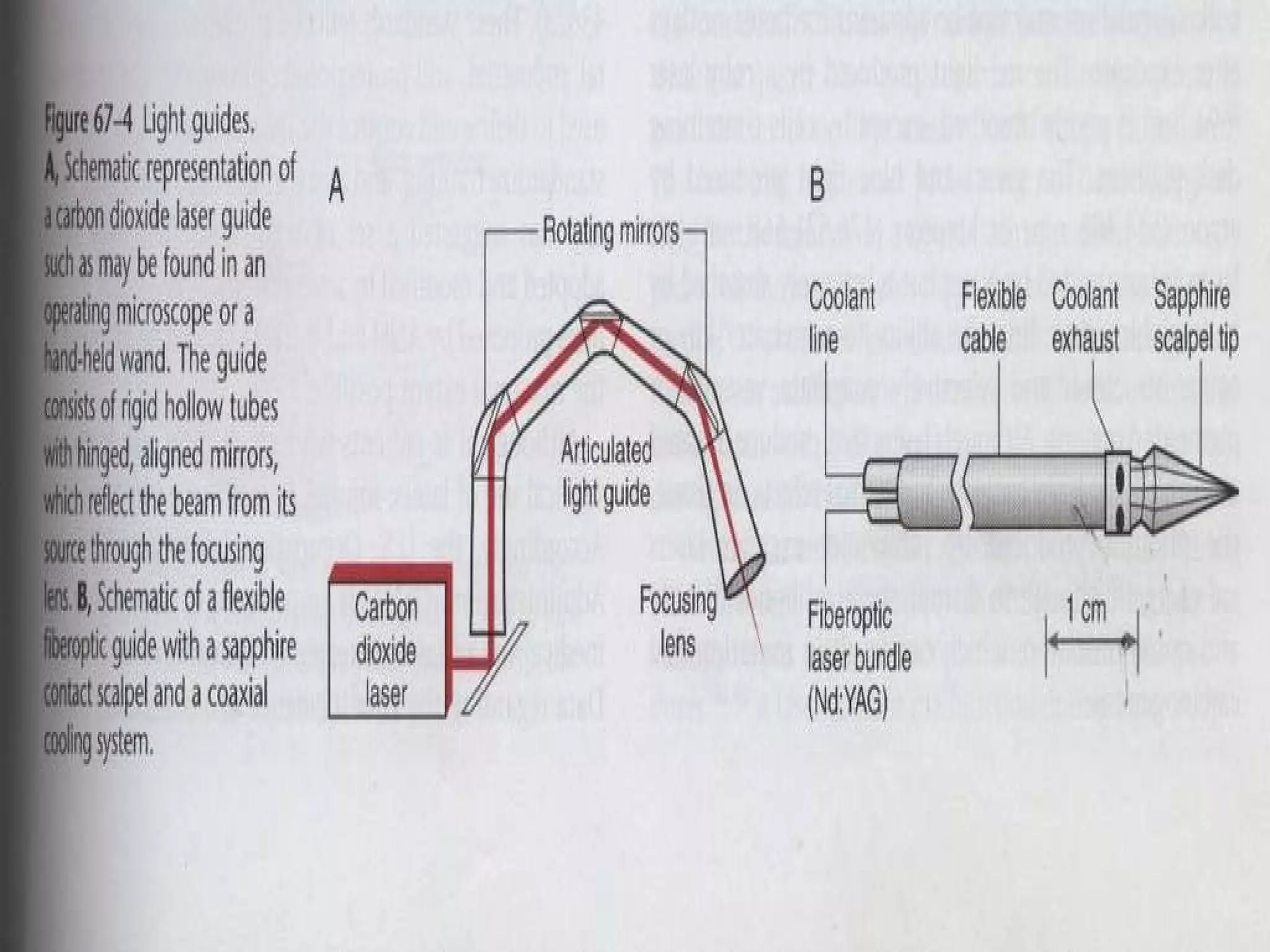
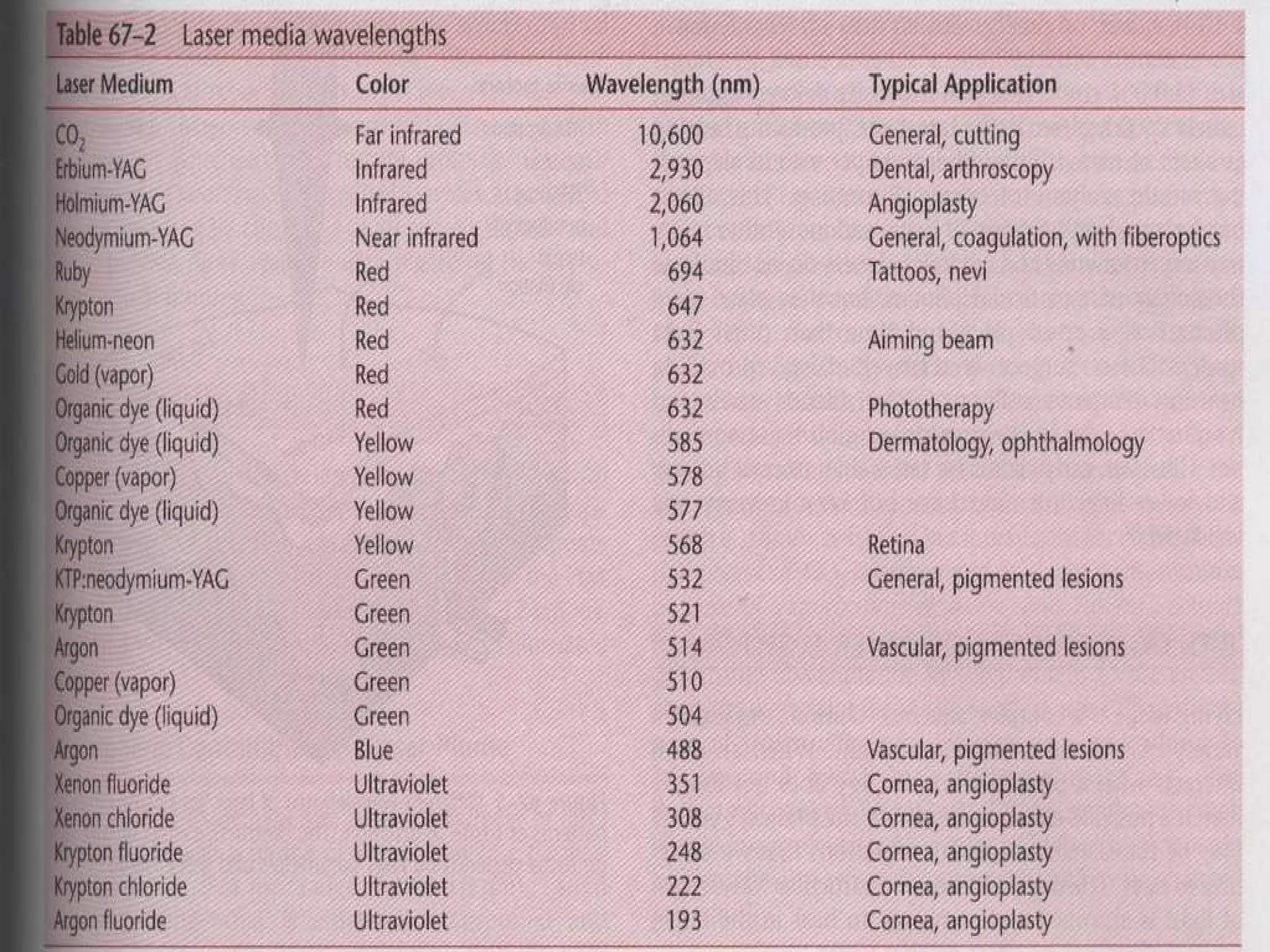
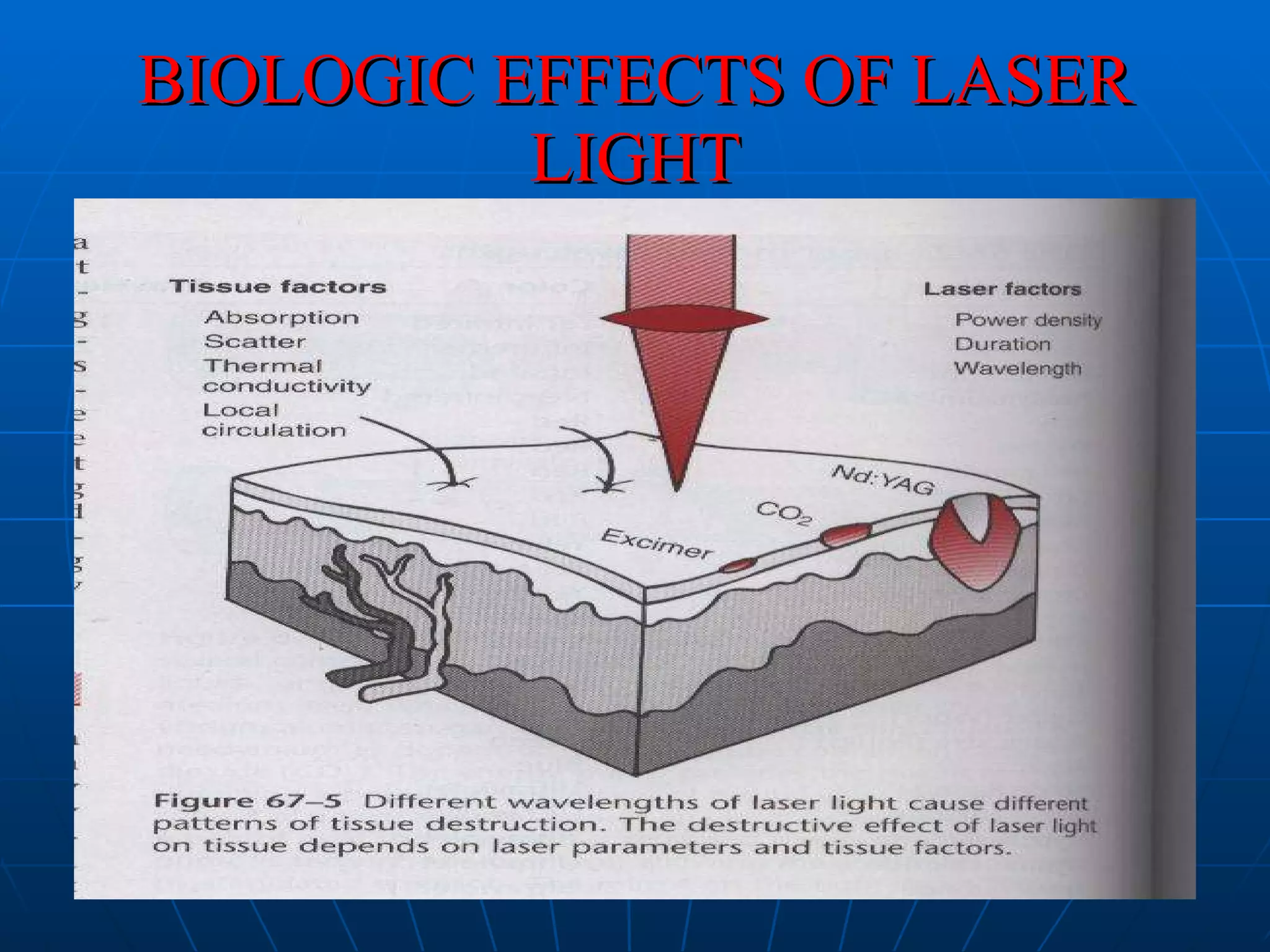
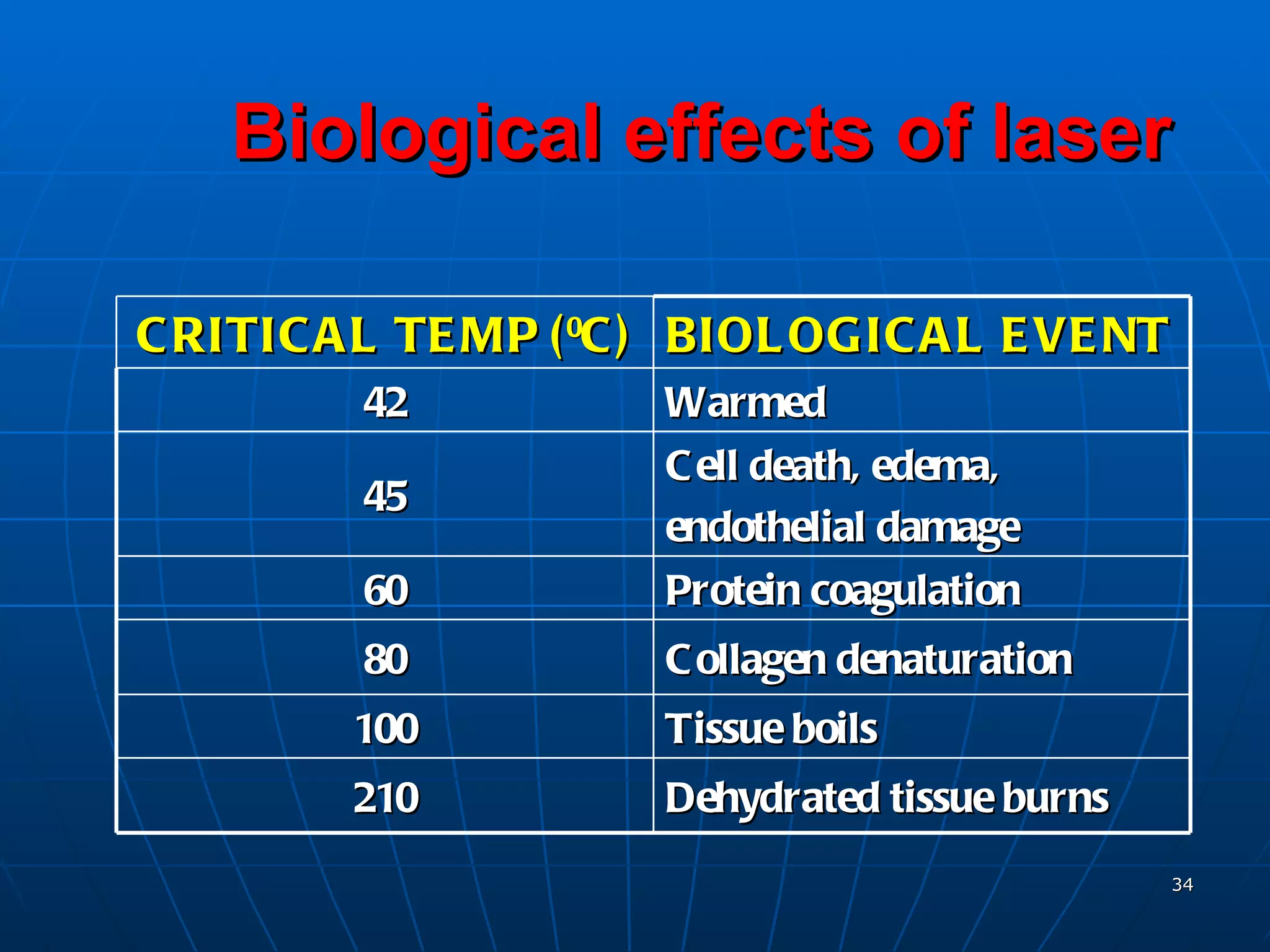
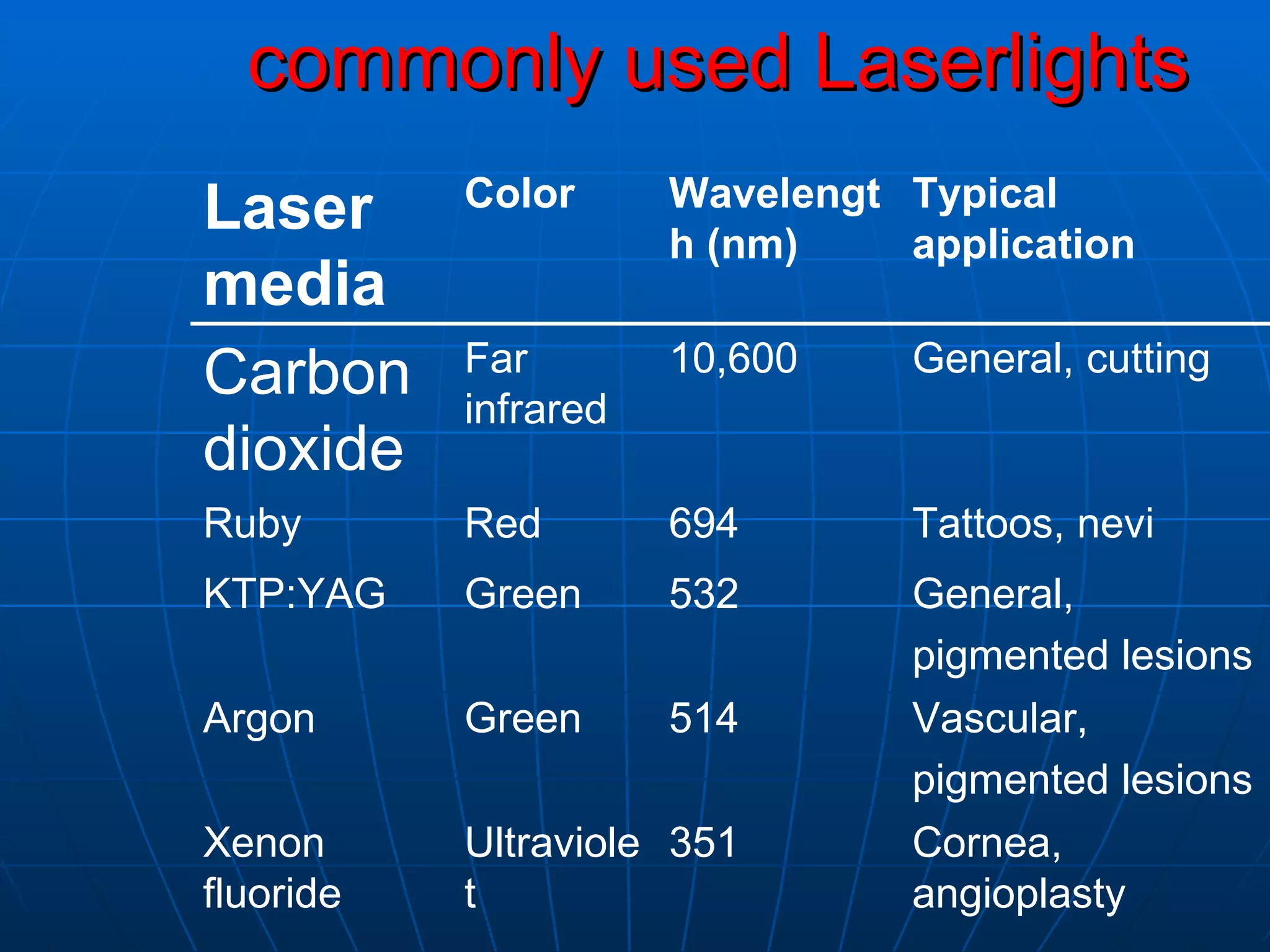









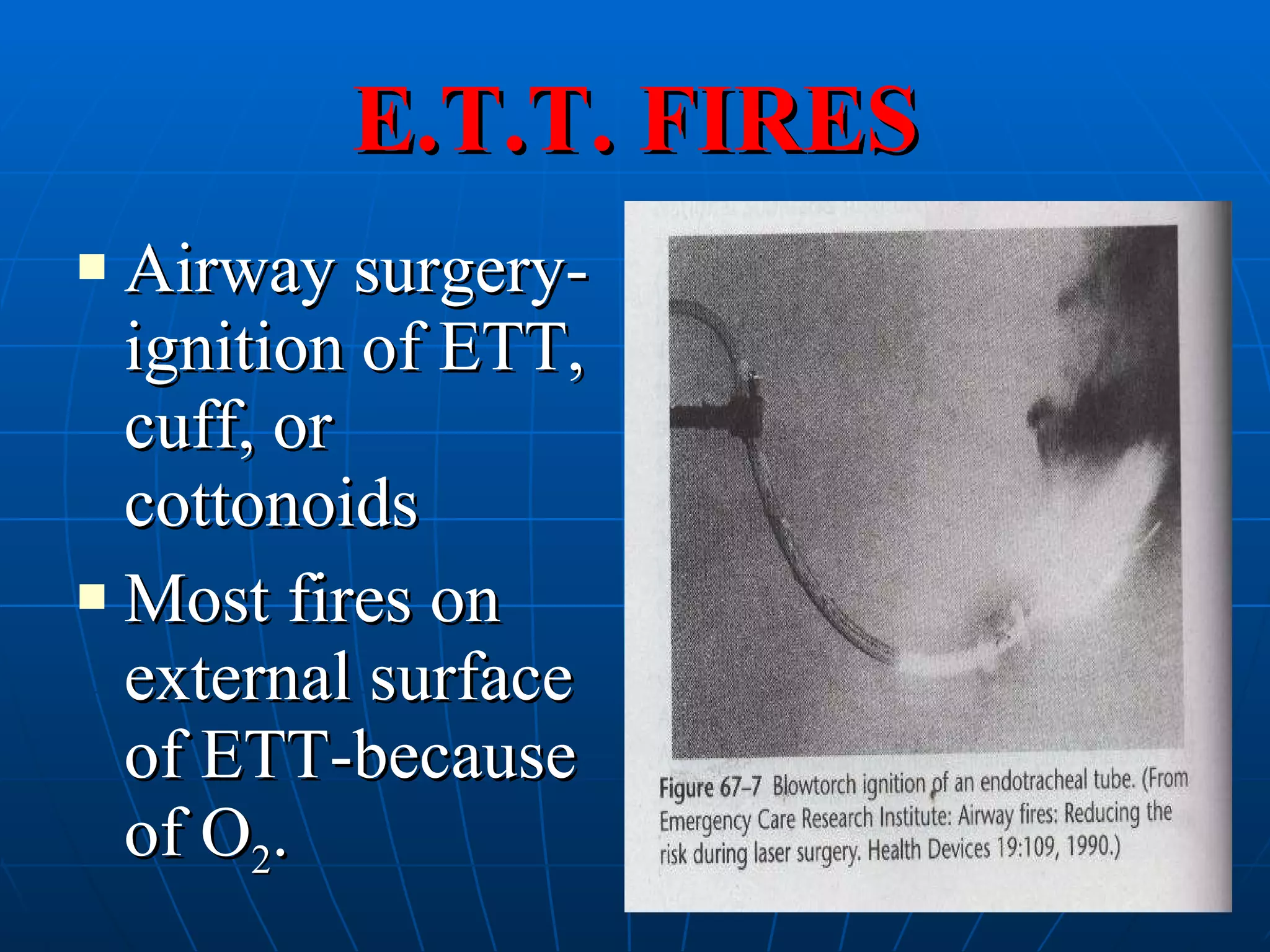




The document discusses lasers and their applications in anaesthesia and surgery. It provides a brief history of lasers, explaining their basic physics and properties. It describes different types of lasers used in medicine like CO2, Nd:YAG, and argon lasers. It discusses biological effects of laser light and various clinical applications of lasers. It also outlines safety considerations for lasers, including protection of the eyes, endotracheal tube fires, and protocols for managing laser-related hazards and emergencies.











































































































