Downloaded 25 times



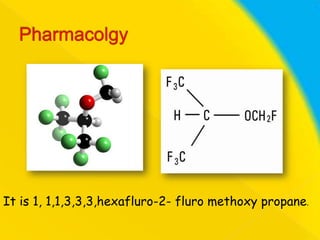
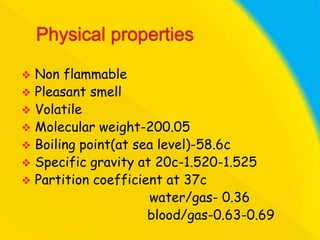
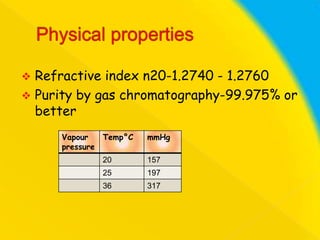
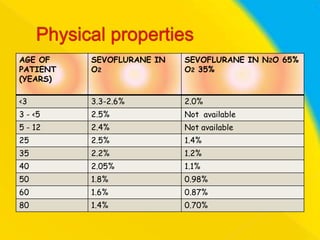








This document discusses the history, properties, uses, advantages and disadvantages of the inhalational anaesthetic Sevoflurane. It provides details on its development in the 1960s, approval for use in 1994 and pharmacological properties. Sevoflurane is highlighted as having advantages for neuroanaesthesia due to its minimal effects on intracranial pressure and cerebral blood flow. While it provides rapid induction and recovery, disadvantages include potential to trigger malignant hyperthermia and other side effects. The document reviews several studies comparing Sevoflurane to other agents.



































































