Downloaded 547 times
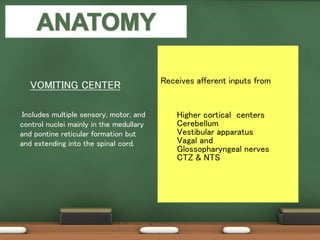
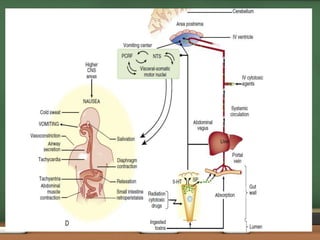
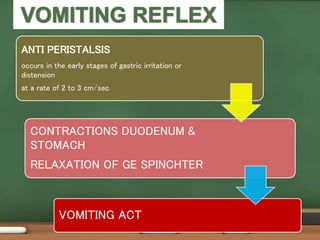
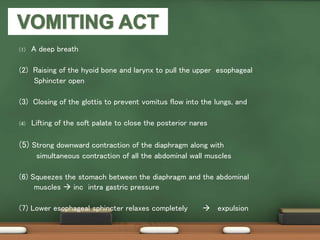
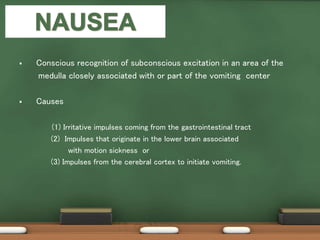

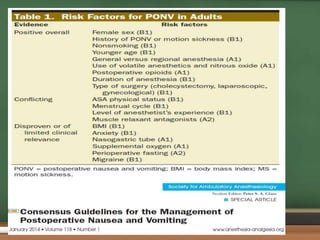


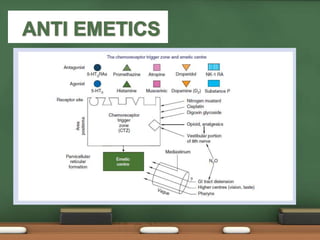





(1) Postoperative nausea and vomiting (PONV) is a common complication following anesthesia and surgery, with incidence rates of 22-38% for nausea and 12-26% for vomiting. (2) The vomiting center located in the brainstem plays a key role in coordinating the vomiting reflex in response to various emetogenic stimuli. (3) Identifying patient, anesthesia, and surgery risk factors can help determine those at higher risk of PONV and guide prophylaxis.





























































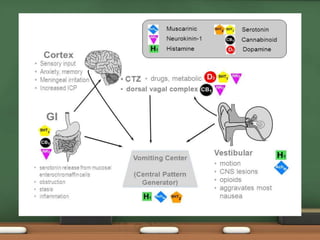
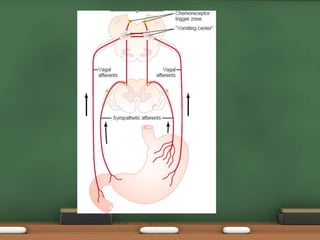
![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














