Downloaded 245 times

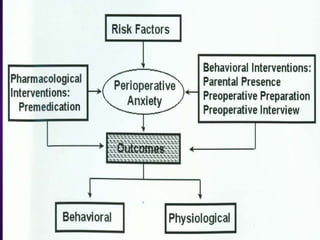


























Modern Trends in Paediatric Preparation and Premedication discusses: 1. Various risk factors for pre-op anxiety in children and interventions like behavioral and pharmacological approaches. 2. Psychological effects of surgery and anesthesia on children and the importance of pre-medication. 3. Guidelines for monitoring patients under sedation and different levels of sedation. 4. Common drugs used for pre-medication like midazolam, ketamine and fentanyl, their doses, routes of administration and potential complications."










































































































