Downloaded 81 times


















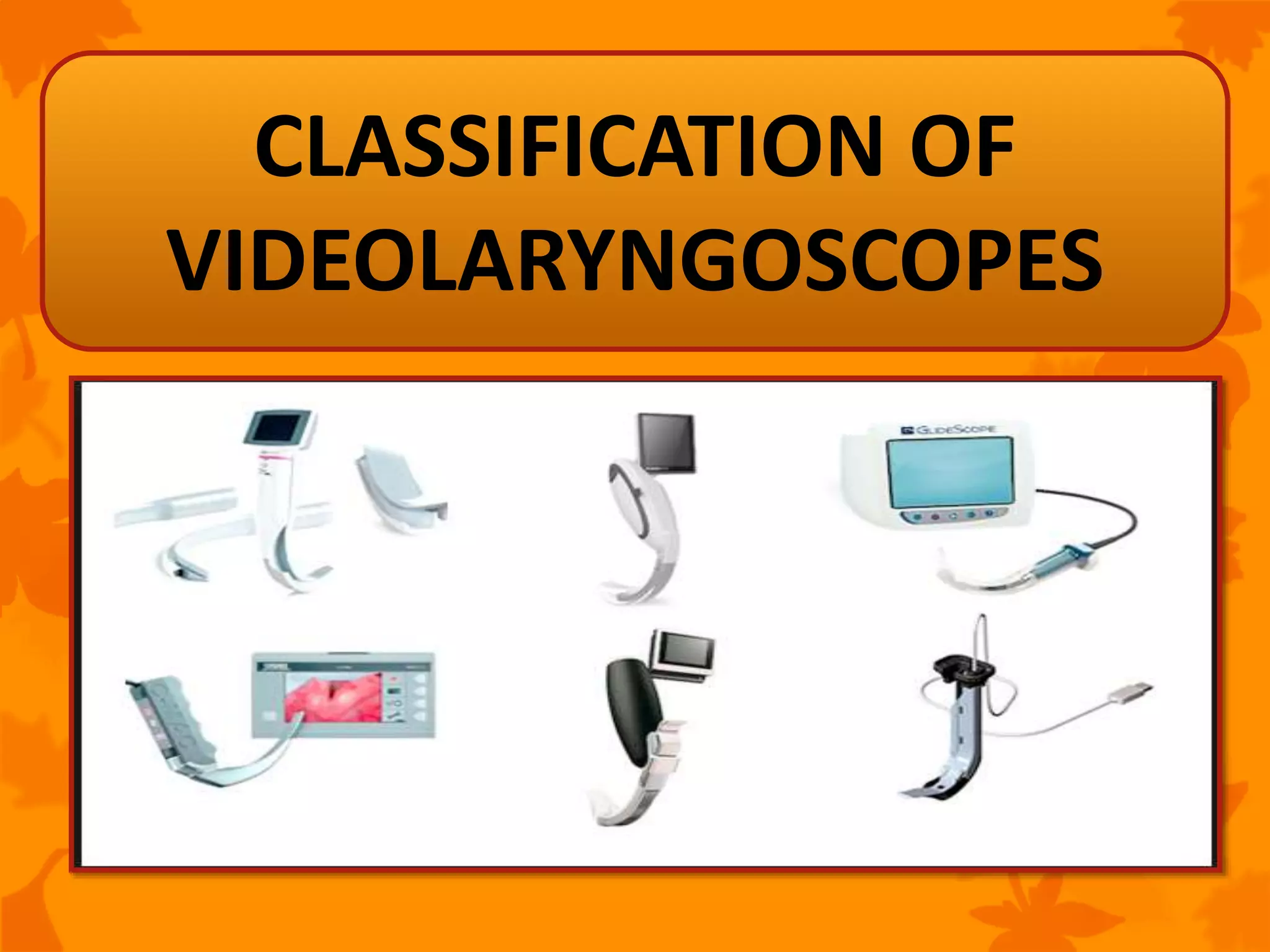







































This document provides an overview of videolaryngoscopes for tracheal intubation. It begins with an introduction to the topic and then describes several key advantages of videolaryngoscopy over direct laryngoscopy. The document proceeds to discuss characteristics of ideal videolaryngoscopes and the process of videolaryngoscopy-aided tracheal intubation. It also provides a classification and description of popular videolaryngoscope devices like GlideScope, McGrath, C-MAC, and others. Studies finding benefits of select videolaryngoscopes in difficult airway scenarios are also summarized.























































































