Downloaded 463 times















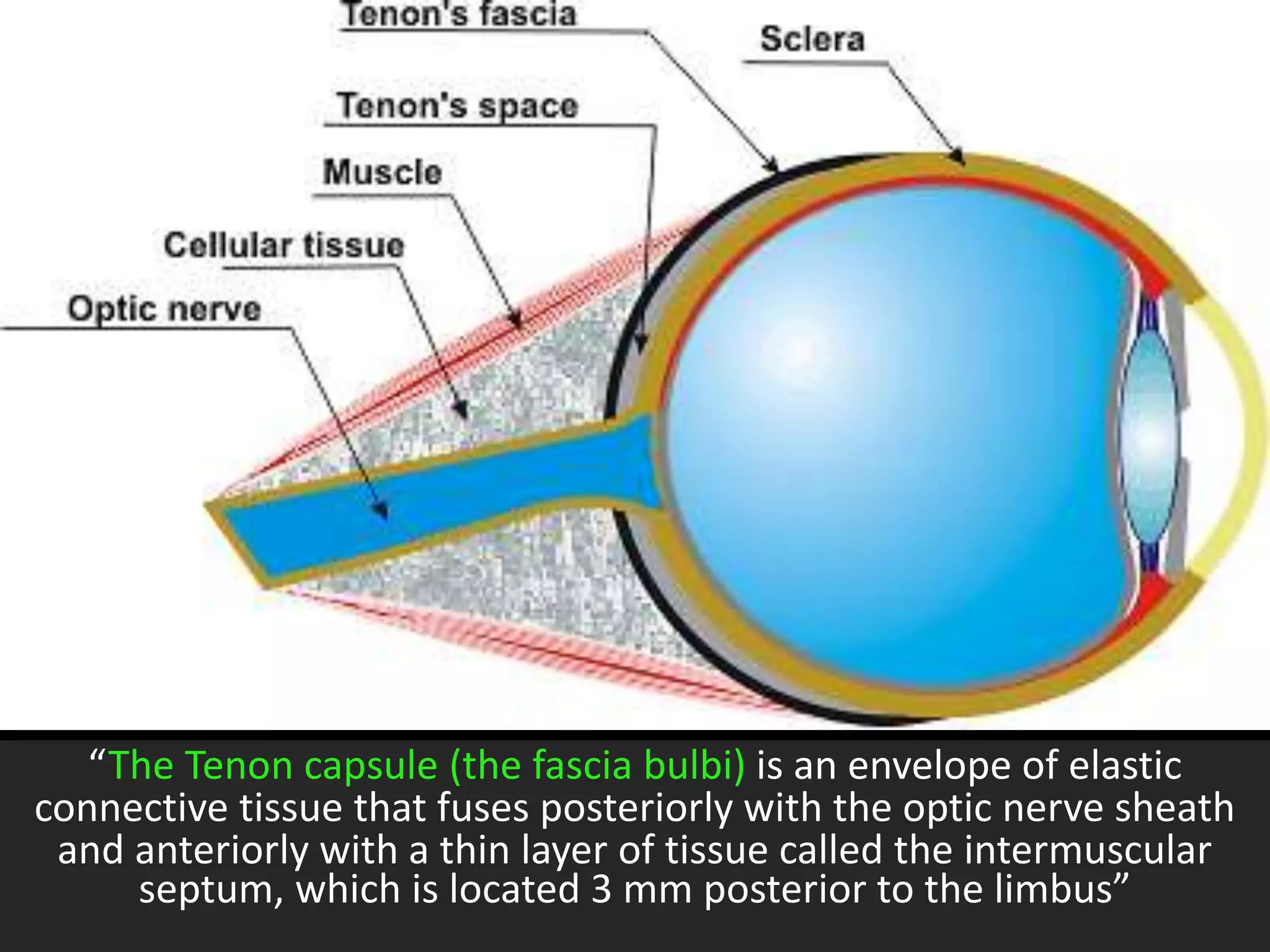
































































1. The document reviews anatomy of the orbit and surrounding structures relevant to ophthalmic anesthesia. It describes nerves, muscles, vasculature and layers within the orbit. 2. Various local anesthetic agents and their properties are discussed. Common techniques for ophthalmic anesthesia including topical, subconjunctival, intracameral, peribulbar, retrobulbar, and facial nerve blocks are explained. 3. Risks associated with different techniques like retrobulbar hemorrhage, globe perforation, and brainstem anesthesia are outlined. The document provides an overview of orbital anatomy and ophthalmic anesthesia techniques and considerations.











































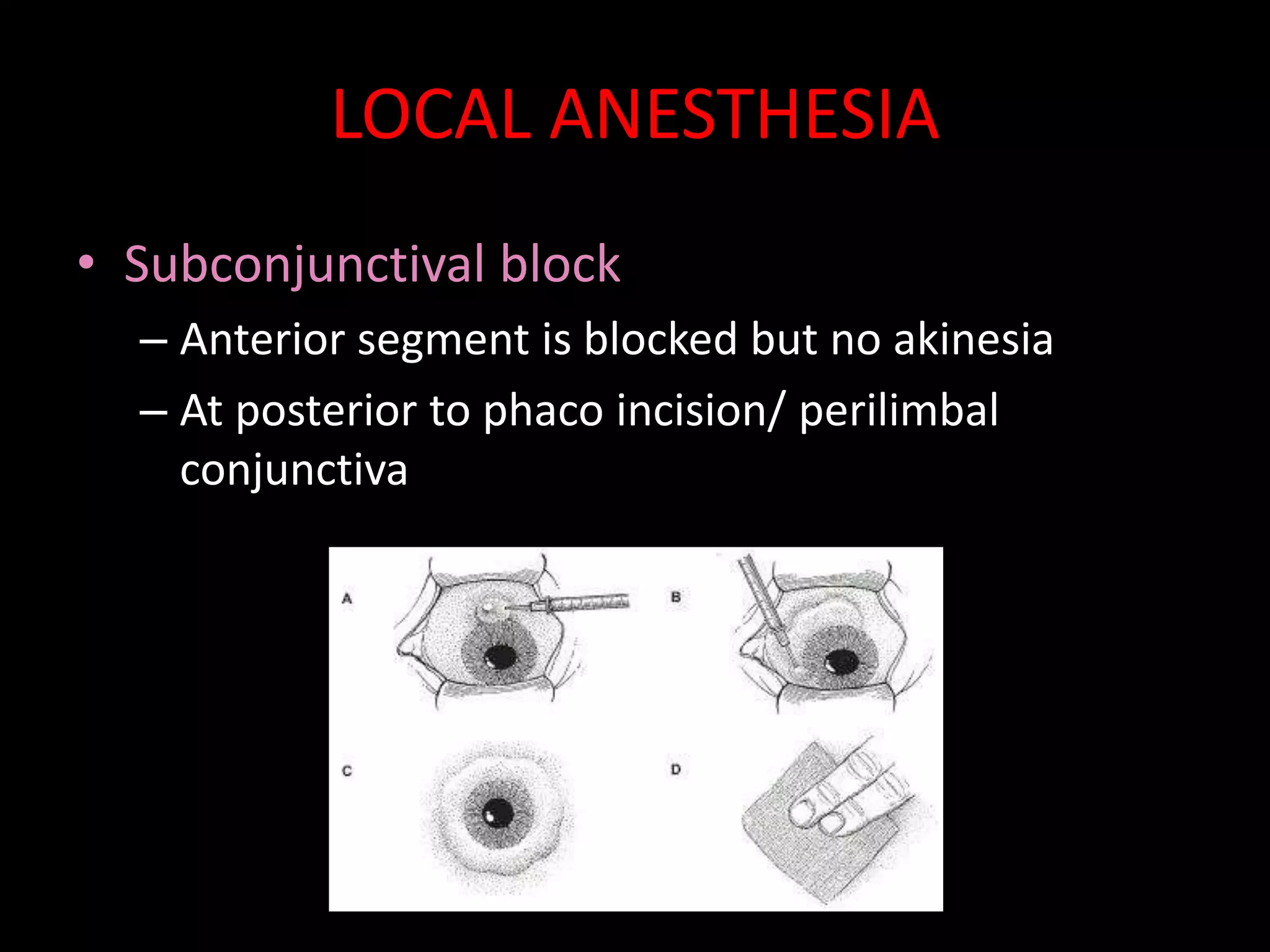
![DR RUTUJA OCULAR ANAESTHSIA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drrutujaocularanaesthsiaautosaved-250415072038-4ff80b96-thumbnail.jpg?width=640&height=640&fit=bounds)






































