Downloaded 1,324 times



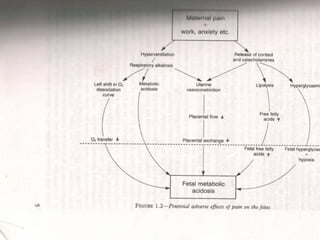
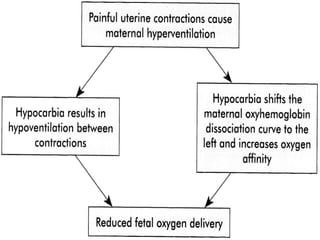
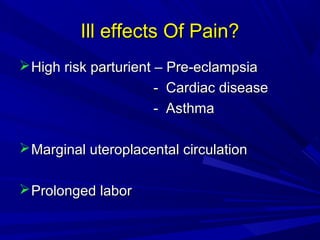
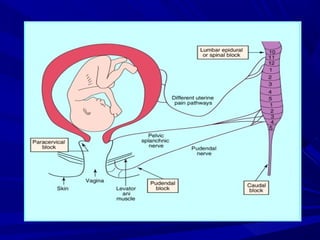

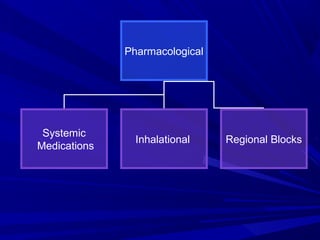


This document discusses the history and physiology of labor analgesia. It provides an overview of the controversy around pain relief during labor and outlines both non-pharmacological and pharmacological options. Regional techniques like epidural analgesia are highlighted as the most effective methods with minimal effects on the fetus when used properly. The goals of labor analgesia and factors to consider when selecting drugs and techniques are also summarized.























































































