
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Postoperative Complication of DALK
Similar to Postoperative Complication of DALK (20)
More from DiyarAlzubaidy
More from DiyarAlzubaidy (13)
Recently uploaded
Recently uploaded (20)
Postoperative Complication of DALK
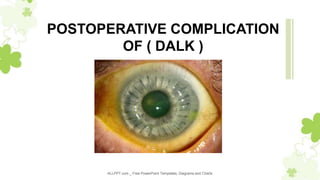
- 1. ALLPPT.com _ Free PowerPoint Templates, Diagrams and Charts POSTOPERATIVE COMPLICATION OF ( DALK )
- 2. DALK procedures • DALK procedures : aim to expose the recipient Descemet membr ane finding a clear plane with uniform thickness (Anwar and Teich mann, 2002; Melles et al., 1999a; Sugita and Kondo, 1997). • DALK can be divided into Descemetic DALK (d-DALK) and pre-De scemetic DALK (pd-DALK). • In d-DALK, the dissection plane is the clear Descemet membrane without any recipient stroma. • In pd-DALK, the dissection plane is above the Descemet membra ne and includes a variable amount of overlying corneal stroma.
- 3. Post-operative complications • Post-DALK pseudo anterior chamber formation ( double AC ). • Corneal stromal graft rejection: Uncommonly, corneal stromal graft rejection has been reporte d after a successful DALK surgery. This complication can present anytime after 3 months post operatively. • Interface haze: occurs in cases where stromal fibers have been left and is apparent in late post -operative follow-up. • Graft dehiscence: Early suture removal may lead to graft dehiscence in some cases. • Recurrence of the original pathology • Decemet’s membrane folds • Interface keratitis: interface left during DALK is a potential dead space • Damage to the iris sphincter muscle resulting in a fixed pupil (more commonly seen in kerato conus patients) (Urrets-Zavalia syndrom) • Pupillary block due to air/gas in the anterior chamber • Suture-related complications: postkeratoplasty atopic sclerokeratitis (PKAS)
- 4. Pseudoanterior chamber • Pseudoanterior chamber Usually seen in the immediate postoperative period and in cases that had an intraoperative perforation of the Decemet’s Membra ne & usually secondary to breaks in the DM . Occasionally, retention of an O VD can lead to a detached DM. • A shallow pseudochamber may be self-limited and may resolve after a few d ays. However, large pseudochambers may persist for weeks and may require surgical intervention. • Surgical correction of pseudoanterior chambers may be performed by injectio n of air or expandable gases such as sulfur hexaflouride (SF6). Possible compl ications of this intervention include pupillary block, iris atrophy, fixed dilated pupils and cataract formation. To prevent these complications, the pupil must be dilated with potency-weak mydriatic prior to injection, followed by anti-gl aucoma medications. If a single injection of air is not enough to correct the p roblem, the process can be repeated until attachment is achieved
- 6. Fixed dilated pupil (Urrets-Zavalia syndrome) • A fixed dilated pupil is not a common complication of PK for kera toconus. Although the precise origin of the syndrome is uncertain • it has been proposed that ischemia of the iris can develop after r aised intraocular pressure. Intracameral air/gas injection to seal int raoperative DM perforation to treat pseudoanterior chamber may cause pupillary block leading to iris atrophy , iridoplegia, posterio r synechia and anterior subcapsular cataract. If it is necessary to l eave an air bubble in the anterior chamber, less than half of the c hamber should be filled with air and/or a peripheral iridotomy sh ould be performed to prevent this complication.
- 8. Interface wrinkling • Folds in the DM following DALK are usually transient and improve over time. The folds are often located peripherally and have no i mpact on vision . • Central folds can decrease the visual acuity likely due to an incre ased level of higher-order aberrations. A mismatch between the d onor button and the recipient bed size is responsible for folds in t he DM; hence, oversizing the donor button by 0.25-0.50 mm is re commended to prevent this complication.
- 10. Interface vascularization and opacification • The occurrence of surface and suture complications may stimulate vascularization of the graft and interface. • This vascularization leads to early suture loosening, appositional p roblems and the need for resuturing. • The primary indication for DALK has an influence on this complic ation. Extensive vascularization may result in lipid and protein extr avasations leading to interface opacification and hence visual acui ty reduction.
- 12. Graft rejection reaction • Although DALK eliminates the risk of endothelial rejection, other t ypes of graft rejection (subepithelial and stromal) may still develo p, with an incidence of between 3 and 14.3%. • The clinical course of subepithelial and stromal graft rejection aft er DALK are very similar to that of PK. Frequent topical steroid us ually leads to reversal of the rejection reactions.Although rejection after LK is easy to control, subepithelial and stromal graft rejectio ns must be treated appropriately to prevent less-severe yet impor tant complications such as suture abscess and graft vascularizatio n that can lead to poor visual outcomes and even lamellar graft f ailure.
- 13. Suture-related complications • such as sterile reactions, early suture loosening, cheese-wiring a nd vascularization,as well as overhanging donor-recipient junction appear to be more common after DALK in comparison to PK . • These complications can be reduced or even prevented by appro priate suture depth (90% of thickness on both recipient and dono r sides), length and tension
- 15. OUR NEIGHBOR ..GLAUCOMA UNIT..
- 17. Shallow AC • Low IOP: microleak from sutures • High IOP : pupillary block by air,retained OVD, malignant glaucom a , swollen graft , steroid responder , zavalia syndrom … goniosco py of other eye to exclude narrow angle
- 19. Risk factors for elevated IOP post DALK included the prior use of patanol 0.1% or ciclosporin eyedrops and the type of topical corticosteroid used following DALK. Musa et al, it has been suggested that the slight rise in IOP after DALK m ay be explained to some degree by the limitations of applanation tonom etry. Since keratoconus is the most important indication for DALK, IOP is l ikely to be underestimated pre-operatively due to the thinner corneas. Af ter DALK, corneas arelatively thick because of the retained predescemetic host stroma in addition to the full donor corneal thickness resulting in the potential for overestimation of IOP. Also, corneal rigidity c hanges after surgery,
- 21. THANK YOU