Downloaded 100 times





























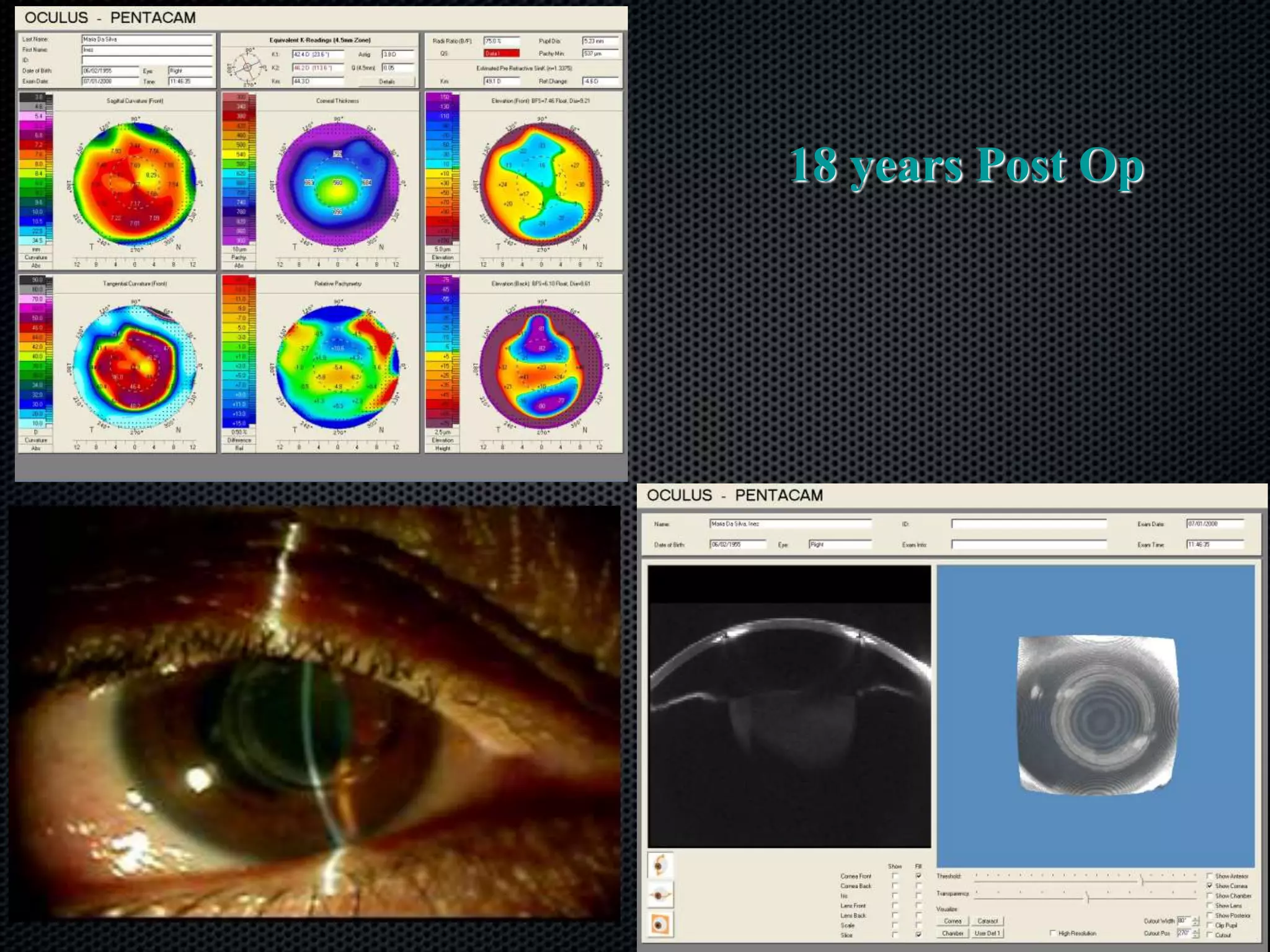
































































































































































The document discusses the Ferrara ring, an intra-corneal implant used primarily for correcting myopia and treating keratoconus, detailing its history, design evolution, and surgical techniques. It explores the indications, patient selection criteria, and clinical outcomes, highlighting the ring's effectiveness and implications for various refractive disorders. Additionally, it compares different nomograms for implantation based on corneal astigmatism and asphericity, emphasizing improvements in surgical strategies over time.























































































