• Cornea isthe chief refractive surface of the eye
• 550 microns thick in the center
• 700 microns in the periphery
• average power of +44 D.
• It is composed of five layers
• epithelium (which is made up of basal columnar cells, wing cells and
surface cells)
• Bowman’s membrane (which is not a true membrane but a condensation
of the superficial stroma)
• stroma which constitutes 90 percent of corneal thickness
• Descemet’s membrane (which is a true membrane)
• endothelium
Indications for refractivesurgery
1. Age >18yrs
2. Refractive stability over 1year
3. Normal corneal topography
4. Discontinuation of contact lens for 1week (soft contact lens )to
3weeks (RGP)preoperatively
5. Healthy ocular surface and adequate tear film formation.
6.
Contraindications
1. Pregnancy andbreast feeding : change
in corneal hydration fluctuation of
the refractive status
2. Abnormal corneal
topography :keratoconus /pellucid
marginal degeneration.
3. Inadequate corneal
topography :keratorefractive
procedures are contraindicated .phakic
IOL’S are better suited
7.
4.Contact sports :boxingflap
dislocation better suited for
SMILE
5.Keloid formation history
surface ablation procedure C/I
6.Co -existing ocular morbidities :
cataract , uveitis and glaucoma.
7.History of herpetic keratitis .
8.
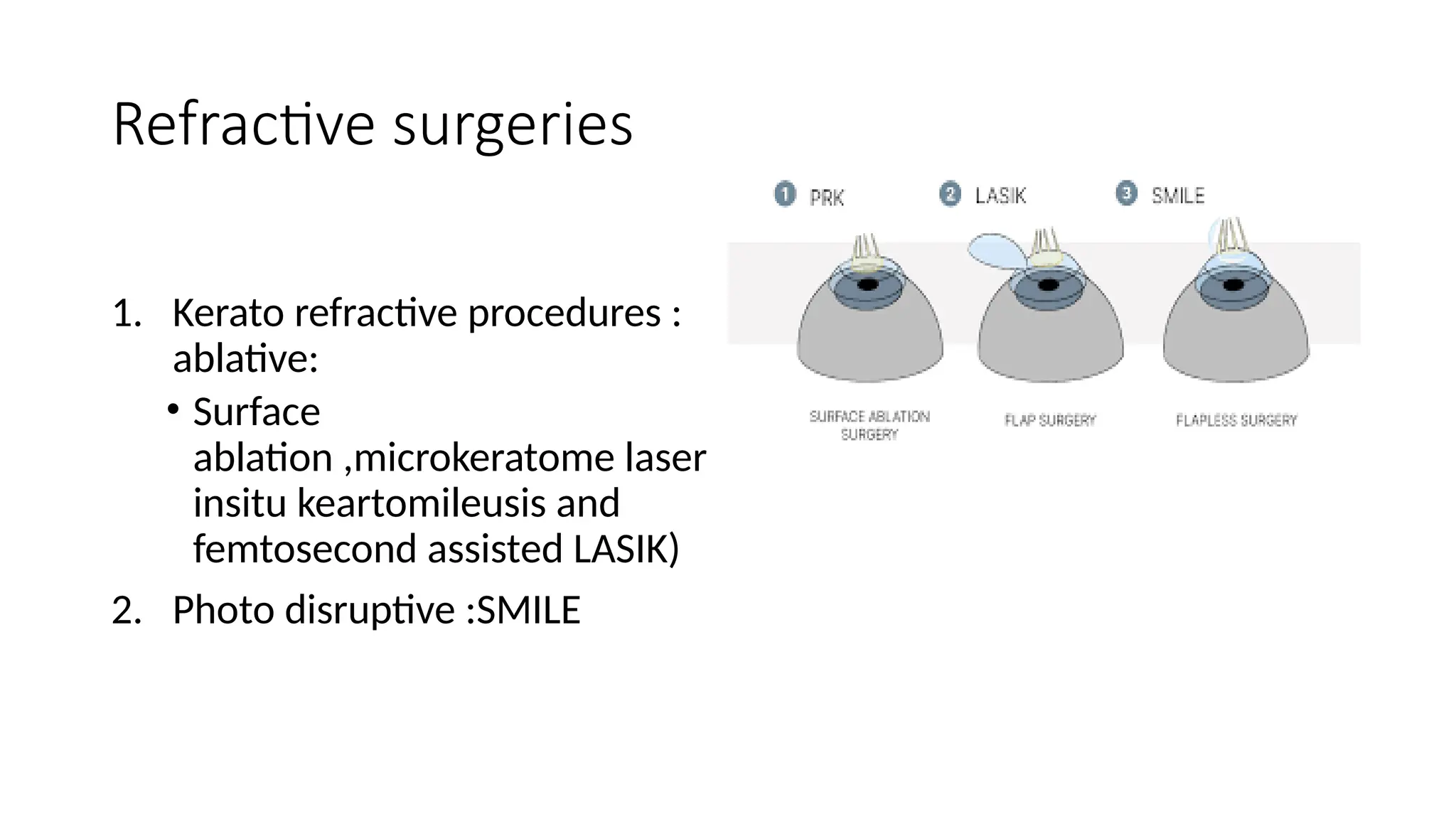
REFRACTIVE SURGERY FORMYOPIA
• CORNEA based procedures:
A)Radial keratotomy :RK
B)LASER based :
1. Photo refractive keratectomy -PRK
2. Laser assisted in situ keratomileusis -LASIK
3. Laser assisted sub epithelial keratomileusis -LASEK
C)Refractive lenticule extraction .-ReLEX
D)Intra corneal ring implantation.-ICR
E)Ortho keratology
• LENS BASED
1.Trifocal IOL
2. Monovision with intraocular lenses
• SCLERAL BASED
1. ACS Anterior scleral sclerotomy
2. Scleral sparing procedures and scleral ablation
3. Scleral expansion .
14.
Clinical evaluation
• Acomplete ophthalmic examination is performed. This includes:
1. Visual acuity
2. Manifest and Cycloplegic refraction assessment
3. Contact lens history
4. Examination of the ocular adnexa
5. Anterior segment slit lamp examination
6. Quantitative and qualitative evaluations of lacrimal
function
15.
7.Evaluation of blinkreflex
8.Intraocular pressure
9.Dilated fundus examination
10.Computerized corneal topography
11.Biometry
12.Pupil diameter
13.Pachymetry
14.Determination of the dominant eye
15.Wavefront measurements.
16.
Slit lamp examination
•Evaluation of the anterior and posterior segments of the eye is
performed.
• the presence of blepharitis/meibomitis is noted and treated prior
to surgery - decrease the risks of infection and interface
inflammation following surgery.
• The presence of superficial punctate keratitis (due to dry eyes).
Schirmer test is done patient counseling that refractive
surgery may worsen the dry eye disease.
• A punctal plug may be placed prior to or immediately after
surgery.
17.
CHOICE OF REFRACTIVESURGICAL PROCEDURE
• The majority of refractive surgery procedures that are performed for
refractive correction of myopia and hyperopia include:
1. Laser In Situ Keratomileusis (LASIK)
2. Photo- refractive Keratectomy (PRK)
3. Photoastigmatic Keratectomy (PARK)
4. Laser Epithelial Keratomileusis (LASEK).
18.
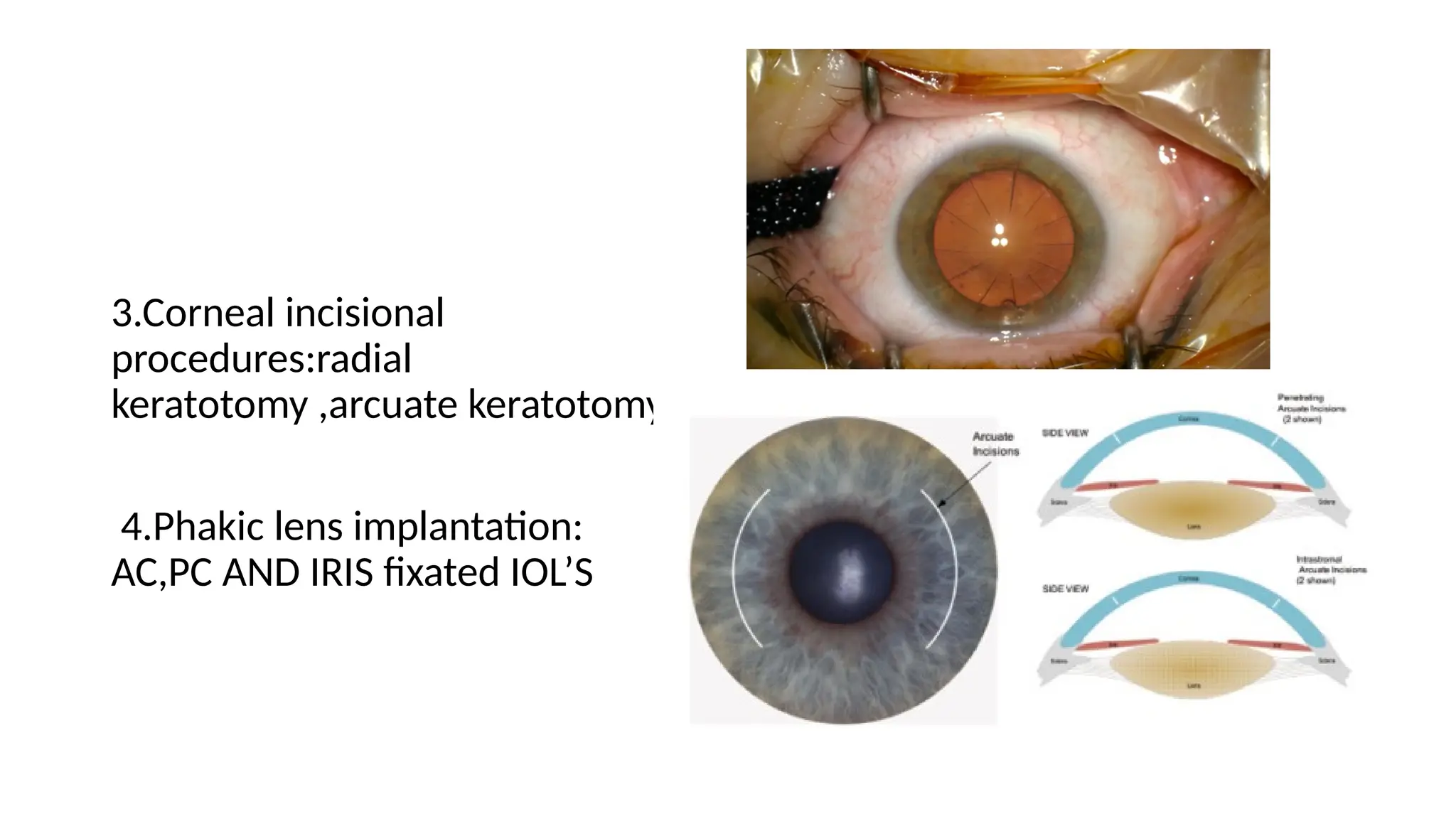
• Incisional refractivesurgical procedures, radial keratotomy (RK) and
astigmatic keratotomy (AK), are associated with progressive hyperopic
shift and structural weakening of the cornea.
• Other refractive surgery procedures include
1. intracorneal ring segments for treatment of low myopia (ICRS)
2. conductive keratoplasty (CK) and laser thermokeratoplasty (LTK) for
low to moderate hyperopia.
19.
• Intracorneal ringsegments (ICRS) or Intacs
inserts (Addition Technology, Inc., Fremont,
CA) are approved for
• patients who have –1.00 D to –3.00 D of
myopia
• with 1.00 D or less of astigmatism
• patients with keratoconus
• with keratectasia.
•
20.
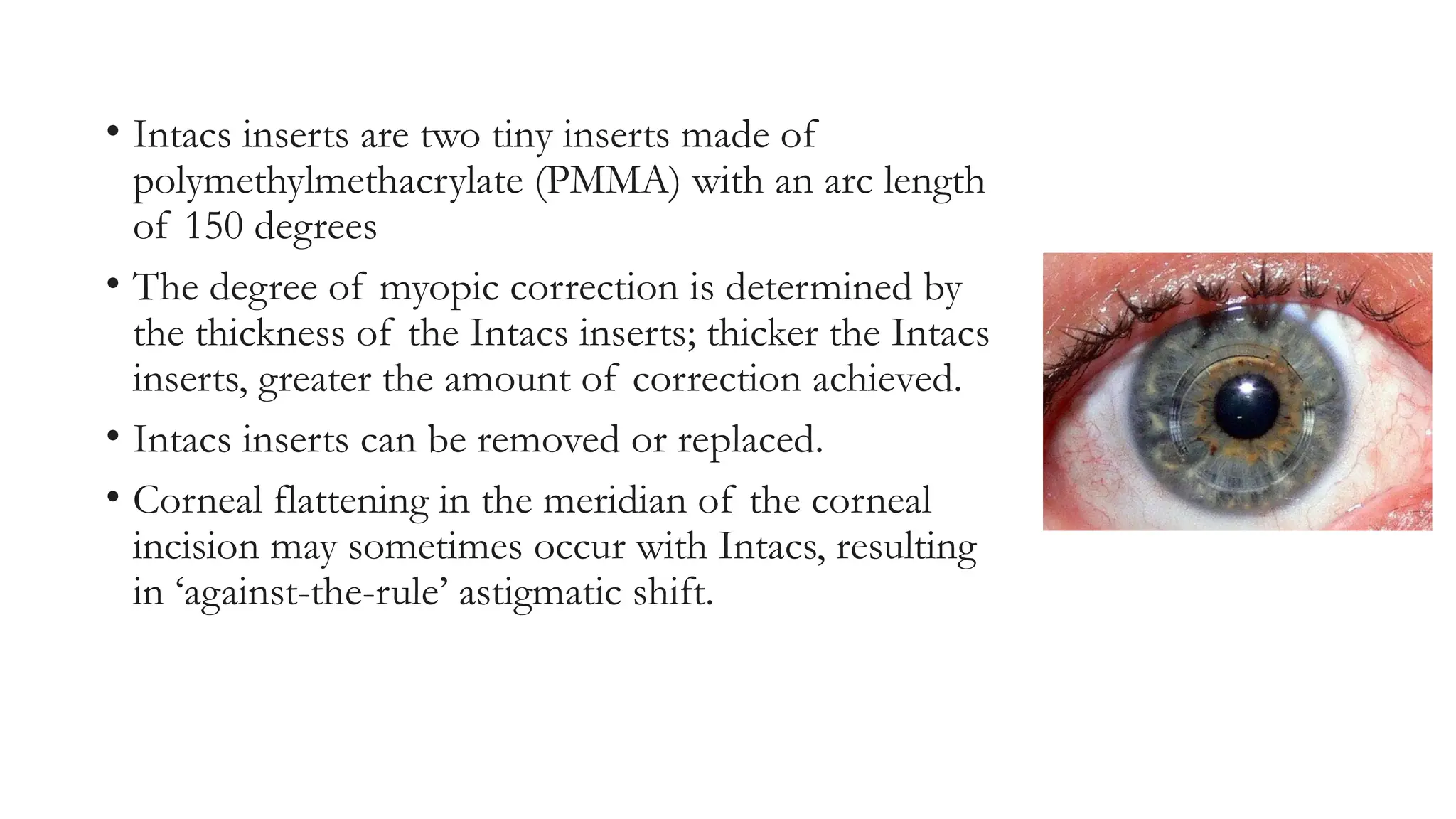
• Intacs insertsare two tiny inserts made of
polymethylmethacrylate (PMMA) with an arc length
of 150 degrees
• The degree of myopic correction is determined by
the thickness of the Intacs inserts; thicker the Intacs
inserts, greater the amount of correction achieved.
• Intacs inserts can be removed or replaced.
• Corneal flattening in the meridian of the corneal
incision may sometimes occur with Intacs, resulting
in ‘against-the-rule’ astigmatic shift.
21.
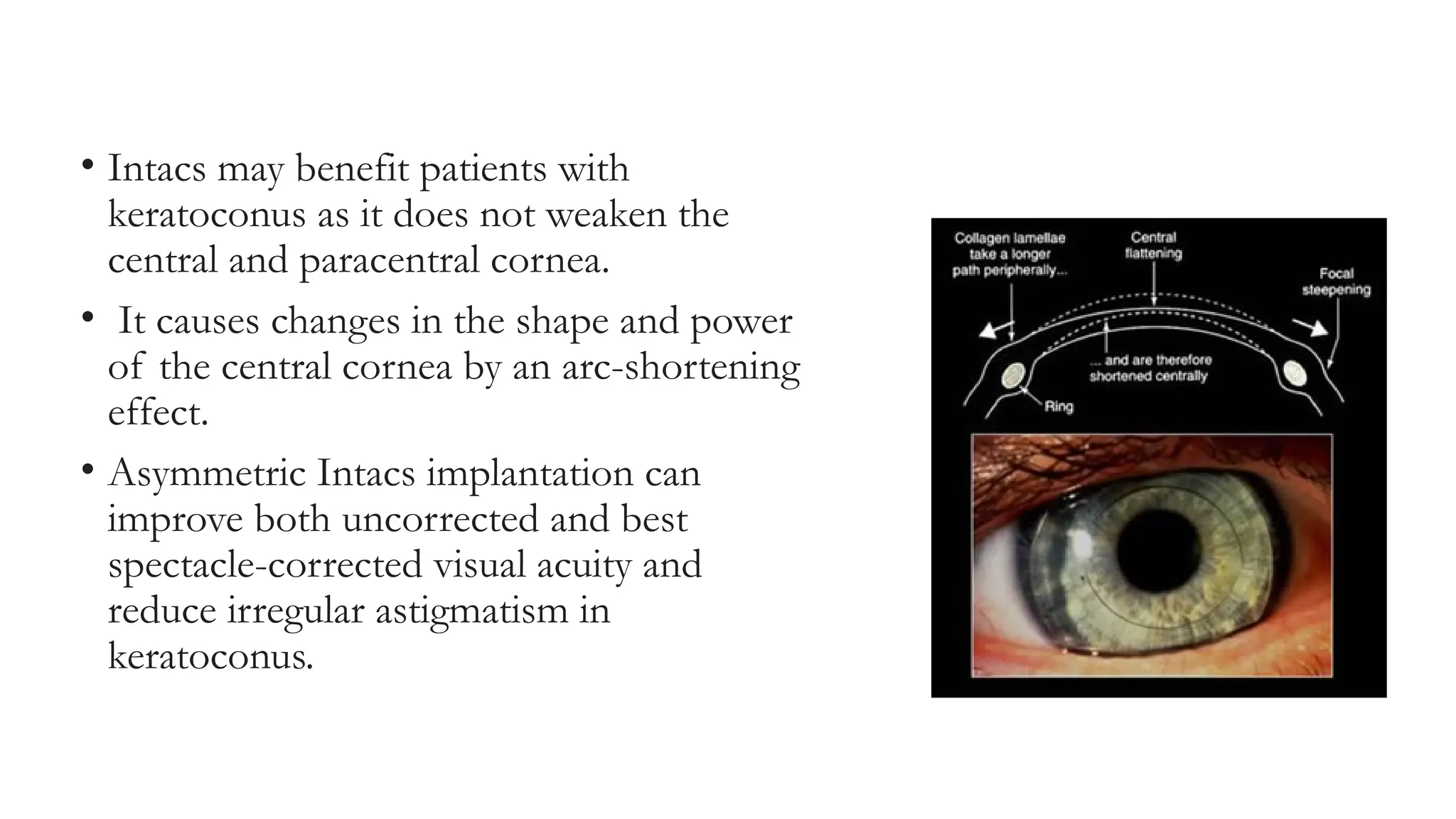
• Intacs maybenefit patients with
keratoconus as it does not weaken the
central and paracentral cornea.
• It causes changes in the shape and power
of the central cornea by an arc-shortening
effect.
• Asymmetric Intacs implantation can
improve both uncorrected and best
spectacle-corrected visual acuity and
reduce irregular astigmatism in
keratoconus.
22.
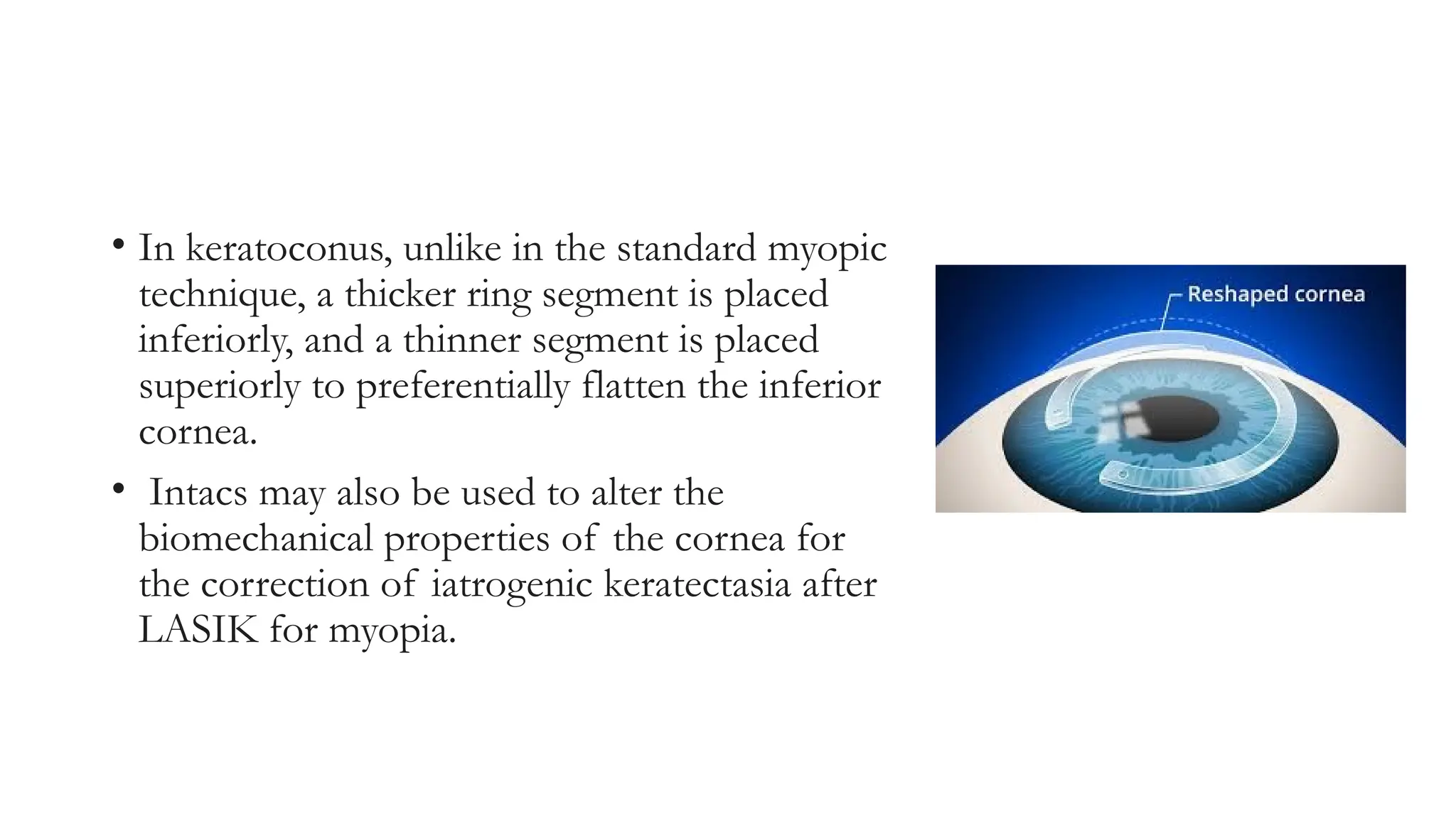
• In keratoconus,unlike in the standard myopic
technique, a thicker ring segment is placed
inferiorly, and a thinner segment is placed
superiorly to preferentially flatten the inferior
cornea.
• Intacs may also be used to alter the
biomechanical properties of the cornea for
the correction of iatrogenic keratectasia after
LASIK for myopia.
23.
LTK
• Laser thermalkeratoplasty is a thermal
technique to shrink peripheral corneal collagen
and thereby steepen the central cornea.
• LTK done in :+0.75 to +2.50 diopters of
hyperopia with not more than 1.0 diopters of
astigmatism.
• is a holmium:YAG laserTwo concentric
rings of eight spots of laser energy is applied
to the periphery of the cornea to gently heat
the corneal collagen and steepen its shape.
24.
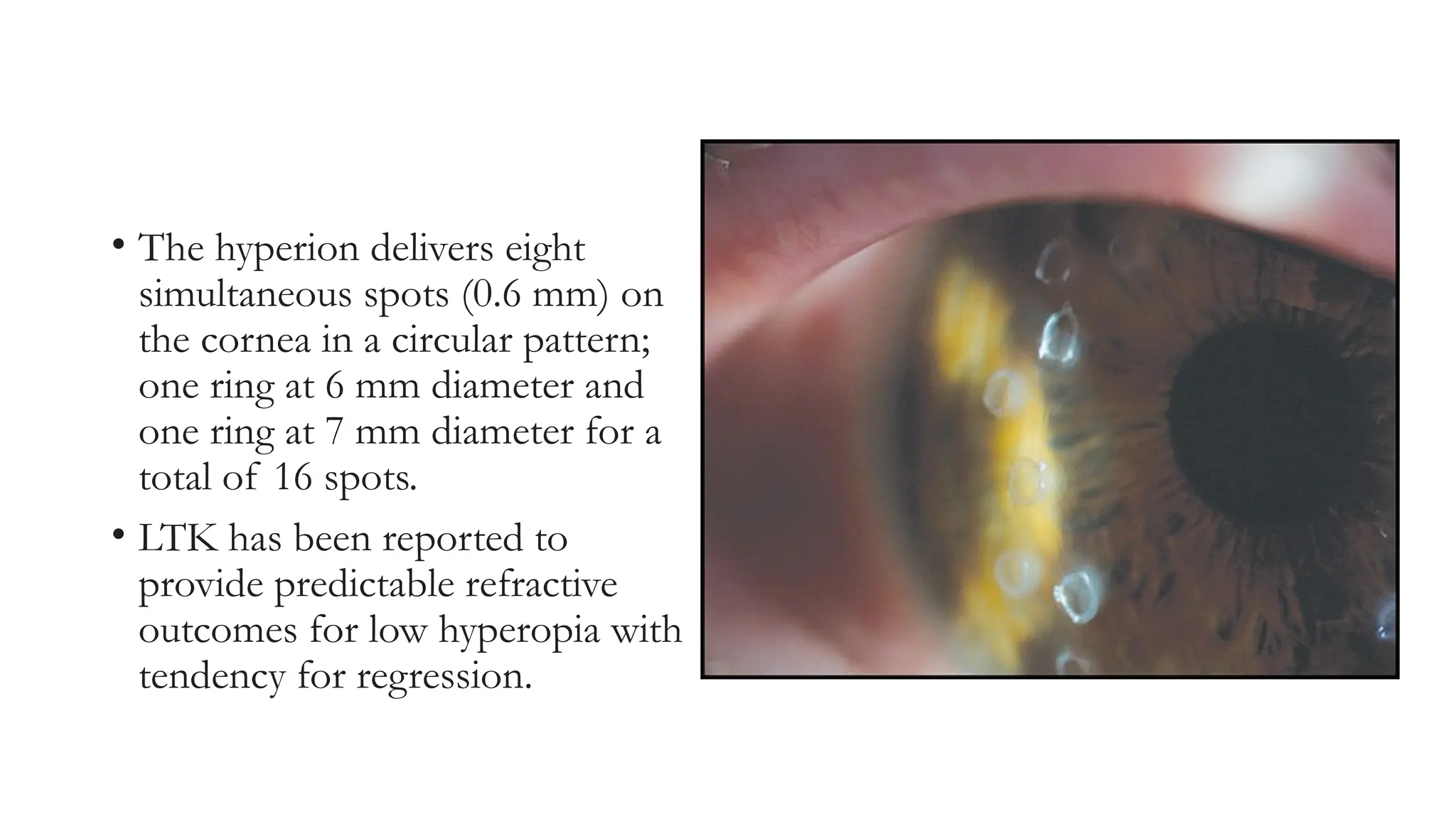
• The hyperiondelivers eight
simultaneous spots (0.6 mm) on
the cornea in a circular pattern;
one ring at 6 mm diameter and
one ring at 7 mm diameter for a
total of 16 spots.
• LTK has been reported to
provide predictable refractive
outcomes for low hyperopia with
tendency for regression.
25.
CK- Conductive keratoplasty
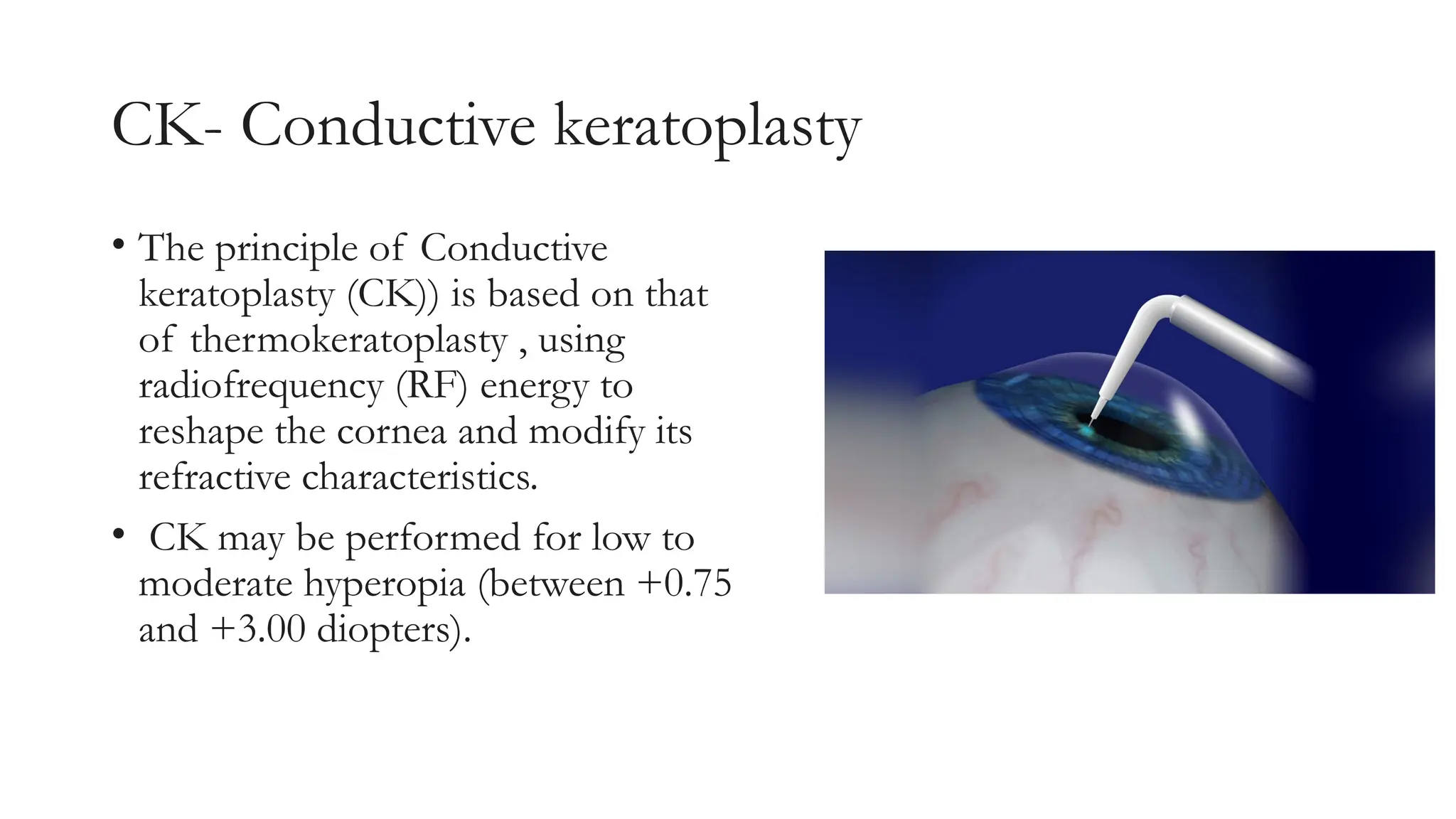
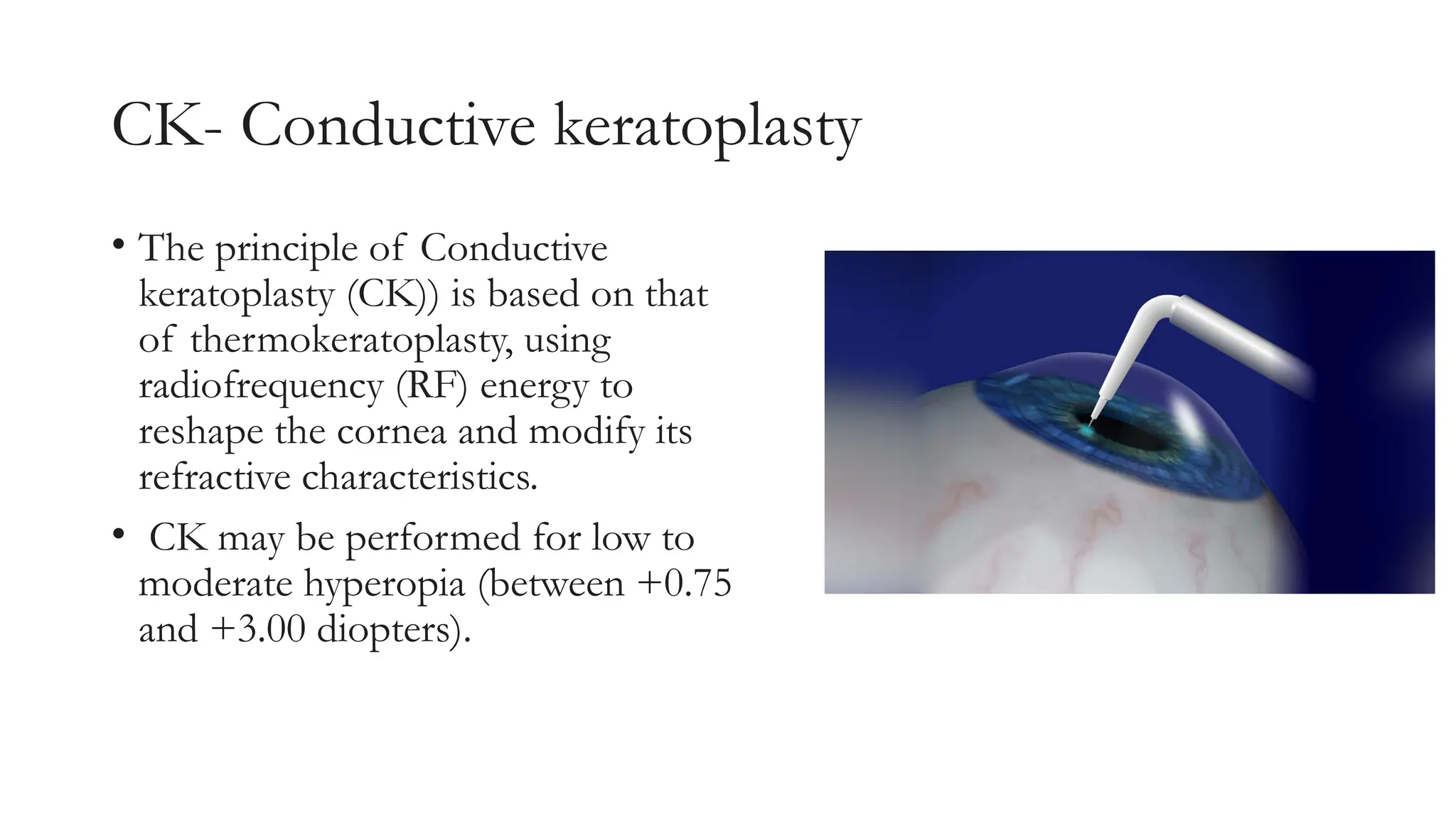
•The principle of Conductive
keratoplasty (CK)) is based on that
of thermokeratoplasty , using
radiofrequency (RF) energy to
reshape the cornea and modify its
refractive characteristics.
• CK may be performed for low to
moderate hyperopia (between +0.75
and +3.00 diopters).
26.
• To performthe procedure, a
handpiece with a Keratoplast tip
delivers controlled RF energy
directly to the corneal stroma in a
ring pattern.
• Conductive keratoplasty creates a
purse-string effect that steepens the
central cornea through a ring of
application spots around the
periphery of the cornea.
27.
Excimer laser
• Principle: ablative photodecomposition
• Uses :ar-f argon flouride
• Electrical energy applied to argon molecule forms excited dimer
(excimer)unstable converted original state and emits photon
that has high energy breaks the collagen break down photo
ablation
• .
29.
Types
• Of excimerlaser
1. Broad beam laserlarge diameter ,higher energy ,lesser pulse and low
repetition state .
2. Flying spot --> small diameter,higher repetition state,higher frequency
3. Slint scanning laser .
• Of ablation profiles :
1. Conventional ablation
2. Wavefront guided ablation
3. Wavefront optimized ablation
4. Topo guided ablation
30.
• Laser proceduresperformed using excimer lasers to correct
refractive errors are of two types:
• Surface Treatment Techniques
• PRK (Photo-refractive keratectomy)
• LASEK (laser-subepithelial keratomileusis)
• Epi-LASIK.
• Lamellar Treatment Techniques
• LASIK using the mechanical microkeratome
• LASIK using the femtosecond laser.
31.
• In PRK,epithelium is removed using a laser
• In LASEK, an alcohol solution is used to abrade the epithelium
• In epi-LASIK, a microkeratome is used to remove a uniform
sheet of epithelium
32.
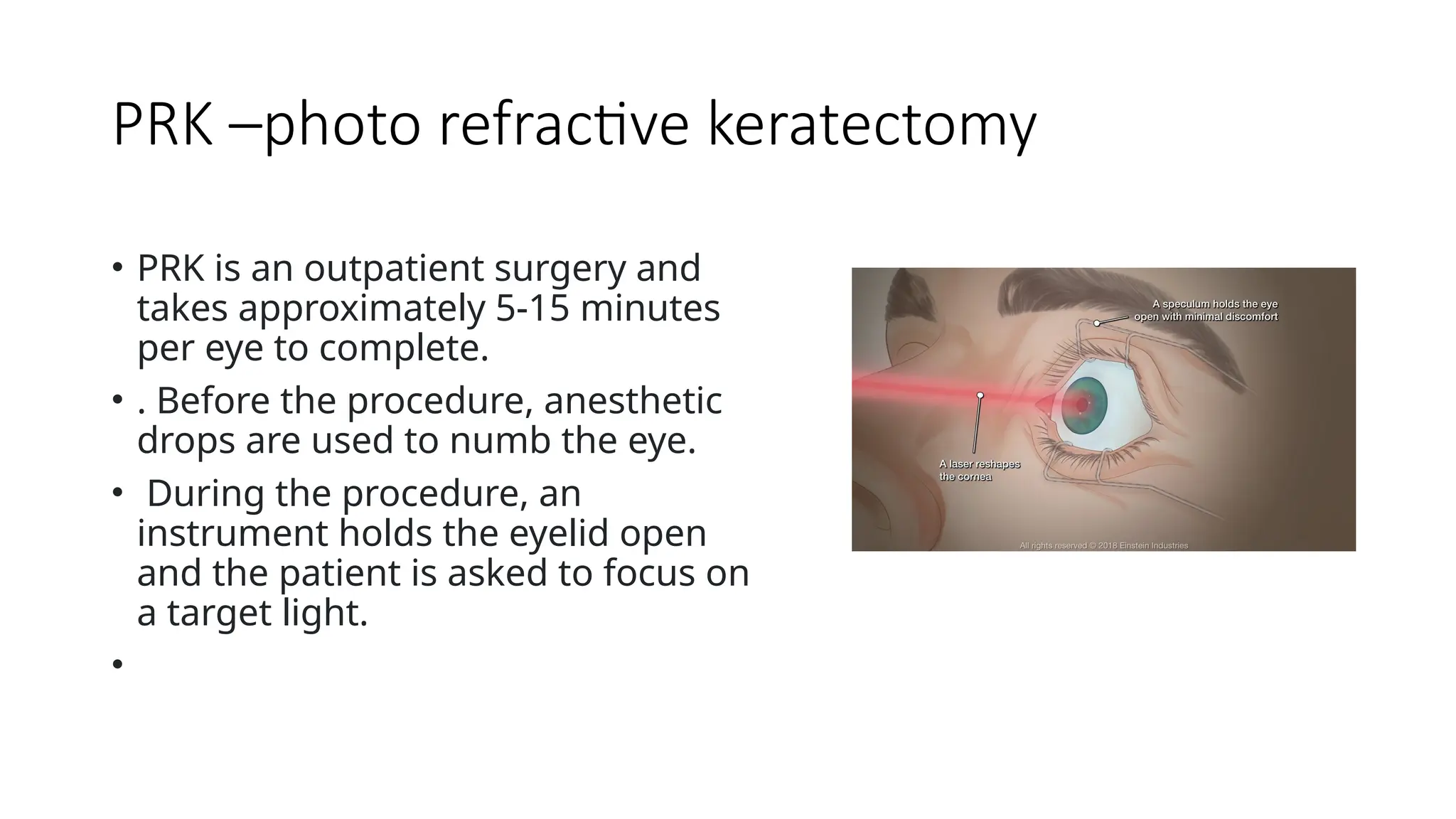
PRK –photo refractivekeratectomy
• PRK is an outpatient surgery and
takes approximately 5-15 minutes
per eye to complete.
• . Before the procedure, anesthetic
drops are used to numb the eye.
• During the procedure, an
instrument holds the eyelid open
and the patient is asked to focus on
a target light.
•
33.
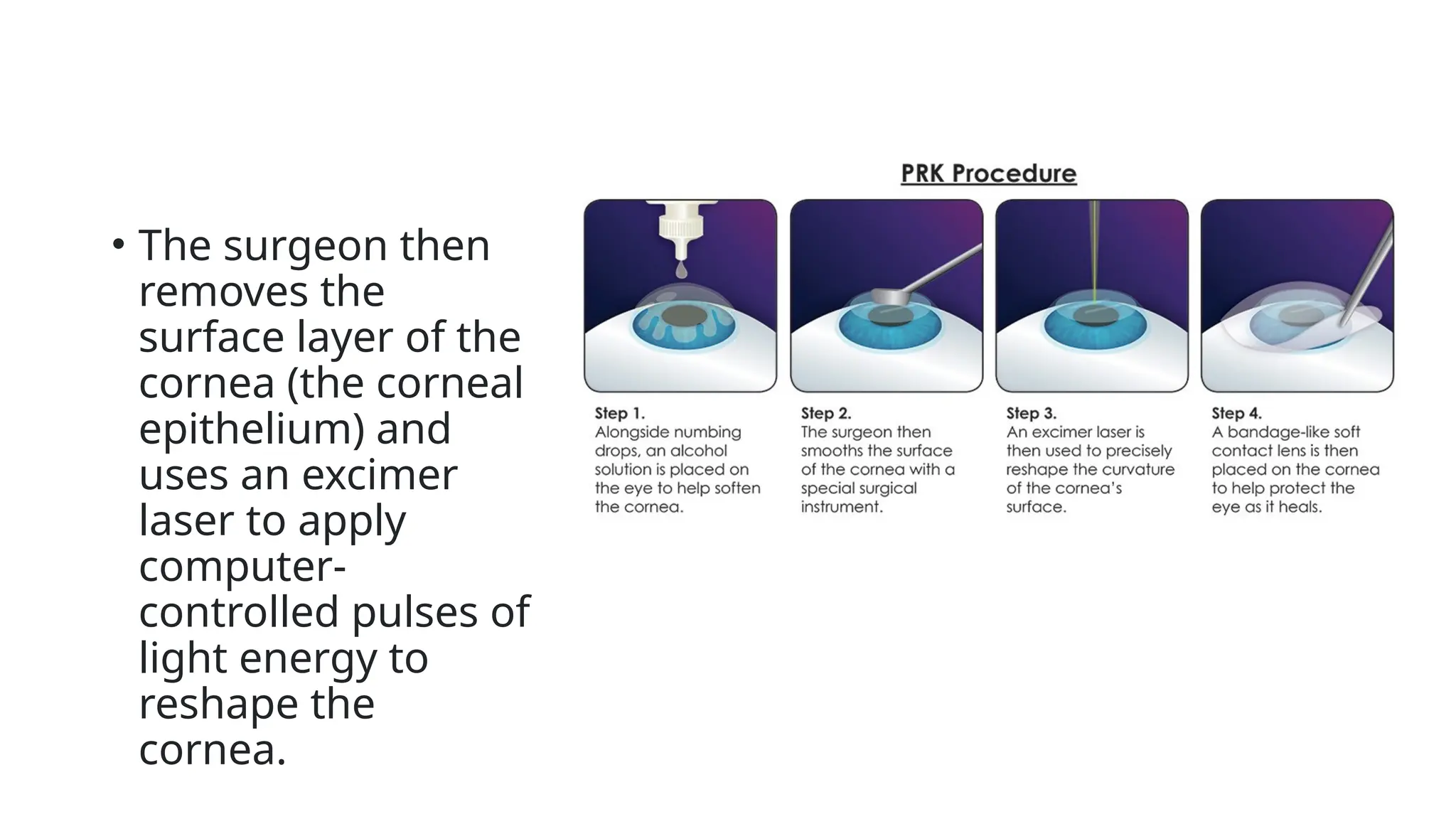
• The surgeonthen
removes the
surface layer of the
cornea (the corneal
epithelium) and
uses an excimer
laser to apply
computer-
controlled pulses of
light energy to
reshape the
cornea.
34.
• Postop:
• softbandage contact lens to protect the cornea as the
epithelial layer grows back over the next 3-4 days.
• Lubricating and antibiotic drops to decrease discomfort,
heal the cornea, and decrease the risk of scar formation and
infection.
• The cornea heals from the edges towards the centre,
forming a “ridge” of epithelium across the pupil where the
healing tissues meet. This ridge usually has formed by the
fourth or fifth day, and it is safe to remove the bandage
contact lens
35.
• The ridgeof epithelium smoothes out over the next 4-6
weeks, the vision will gradually improve.
• The correction is usually considered to be stable by 3-6
months after surgery, at which time an enhancement could
be considered if necessary.
36.
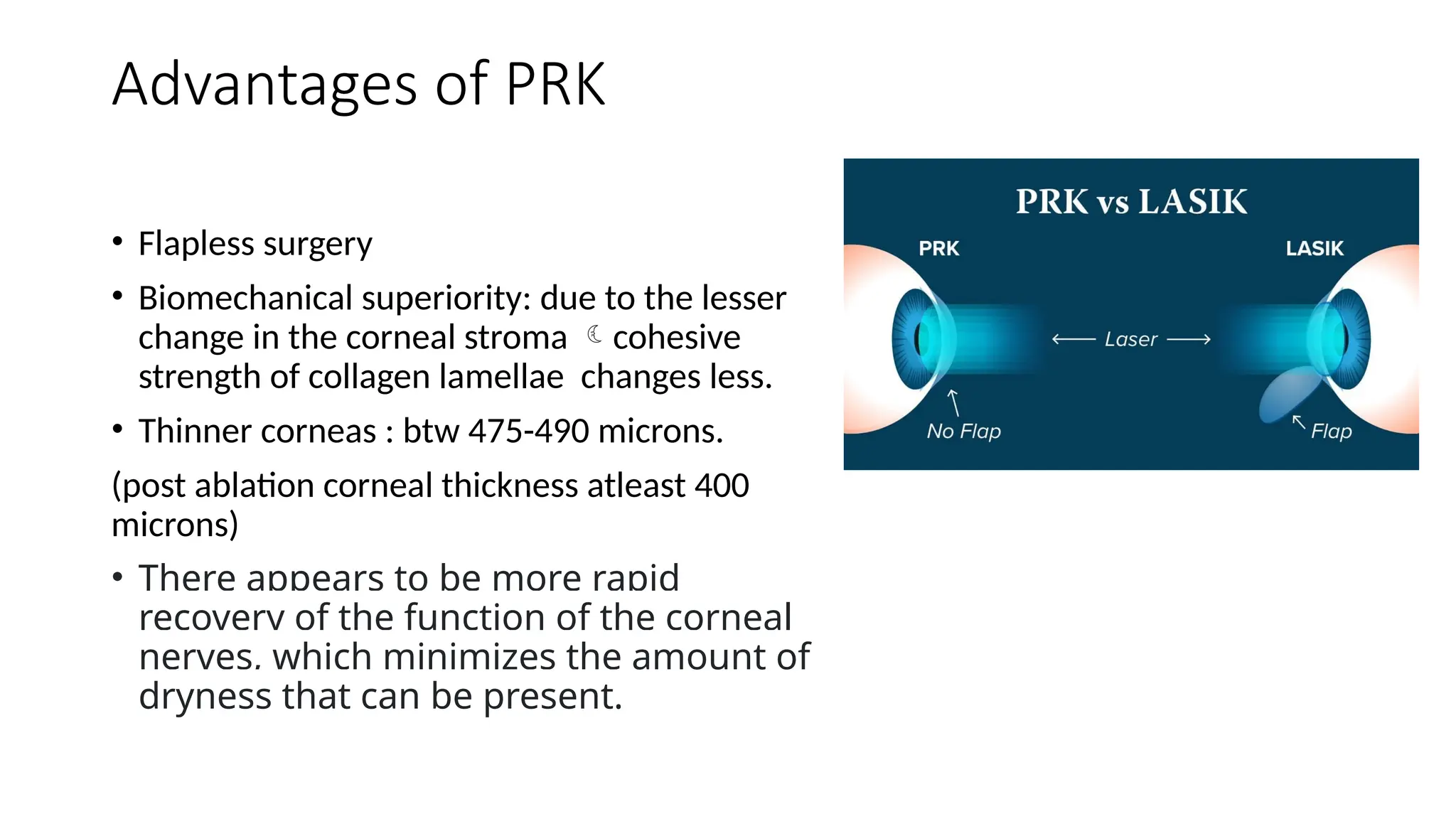
Advantages of PRK
•Flapless surgery
• Biomechanical superiority: due to the lesser
change in the corneal stroma cohesive
strength of collagen lamellae changes less.
• Thinner corneas : btw 475-490 microns.
(post ablation corneal thickness atleast 400
microns)
• There appears to be more rapid
recovery of the function of the corneal
nerves, which minimizes the amount of
dryness that can be present.
37.
Disadvantages
1. Post oppain and discomfort
2. Slow visual recovery
3. Reepithelization+infection and haze
• Haze formation decreased with the use of 0.02%mitomycin
intraoperatively(8-10 seconds per dioptric power correction/30sec for
all dioptric powers)
38.
LASIK
• Preoperative Examination
•Contact lenses must be removed for a minimum of 7 to 14 days
(soft contact lenses) and 3weeks (rigid gas permeable lenses)
prior to the preoperative examination.
• Systemic contraindications :
• auto-immune disorders, collagen vascular disorders, diabetes mellitus
and immunocompromised states.
• pregnant and nursing women should also defer
39.
• ophthalmic contraindicationsinclude
1. active ocular disease or inflammation as in conjunctivitis, scleritis, iritis
or corneal ulcer.
2. Severe dry eye associated with kerato-conjunctivitis sicca or exposure
keratitis is an absolute contraindication.
3. Herpes zoster ophthalmicus or herpetic keratitis especially if active in
the previous six months is at risk for reactivation after exposure to
ultraviolet radiation.
40.
4.Corneal ectasias seenin keratoconus, pellucid marginal degeneration and
keratoglobus also preclude LASIK surgery.
5.Glaucoma, diabetic retinopathy and progressive retinal disease make the
patient unsuitable for a refractive procedure.
41.
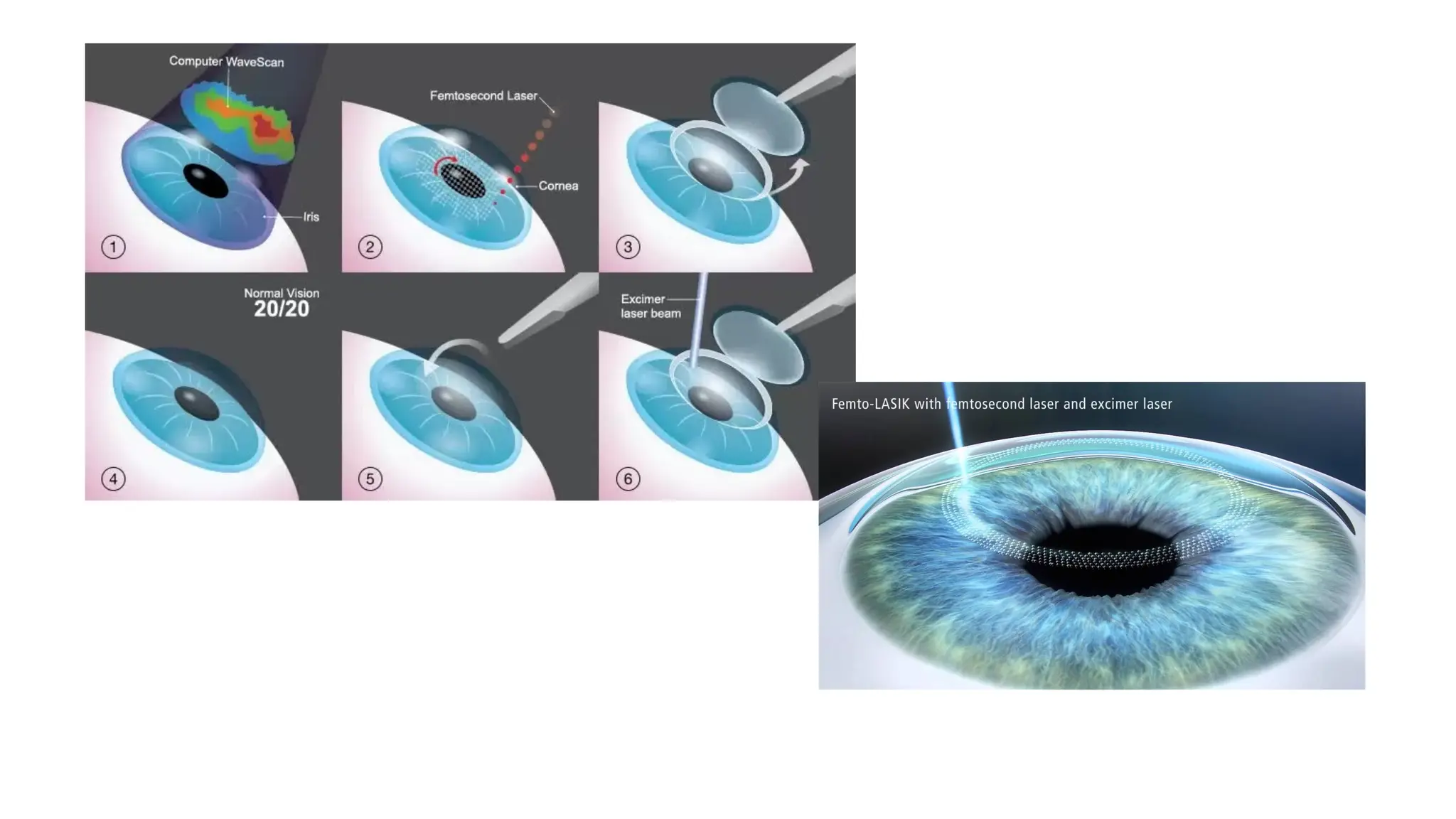
• Lamellar TreatmentTechniques
• LASIK using the mechanical microkeratome
• LASIK using the femtosecond laser
• In lamellar laser techniques, a microkeratome or a femtosecond
laser is used to create a flap.
• The flap is everted on its hinge and the stroma is exposed for
laser ablation.
• After ablation, the flap is reflected back in its original place
where adhesions form within a few hours
43.
Performing the LaserProcedure
• Based on the refraction, corneal topography and wavescan
measurements, the laser treatment plan is made.
• The information is compiled together and the ablation profile is
created keeping a residual bed thickness of atleast 250
microns.
• The laser technique is adopted depending on the amount of
refractive error, the corneal thickness and the ablation depth
required while maintaining the minimum bed thickness.
44.
• The ablationprofile of an excimer laser corrects the spherical
and cylindrical portions of the refractive error with lasers for
myopia removing tissue from the centre of the cornea to make
the cornea flatter
• hyperopic ablations are performed in the corneal periphery to
make the central cornea steeper.
• Aspheric and wavefront-guided ablation profiles treat higher-
order aberrations (HOA) of the eye and thus improve the
patient’s quality of vision.
45.
• Eye trackersmonitor the centre of the pupil and the iris pattern
to prevent de-centered ablations and compensate for normal
saccadic eye movements.
• The ablation procedure stops if the eye tracker cannot locate
the pupil so that incorrect or poorly centered ablations are not
performed.
46.
• Standard LASIKablation parameters are
available, like the Maloney’s tables.
• These charts have the ablation depths
calculated based on the refractive error and
treat the spherical and cylindrical components.
• However, they do not treat the higher order
aberrations (HOAs) and may even induce
them especially during correction of high
refractive errors.
• To avoid this, customized LASIK or C-
LASIK is performed, which integrates
wavefront technology with the laser treatment.
47.
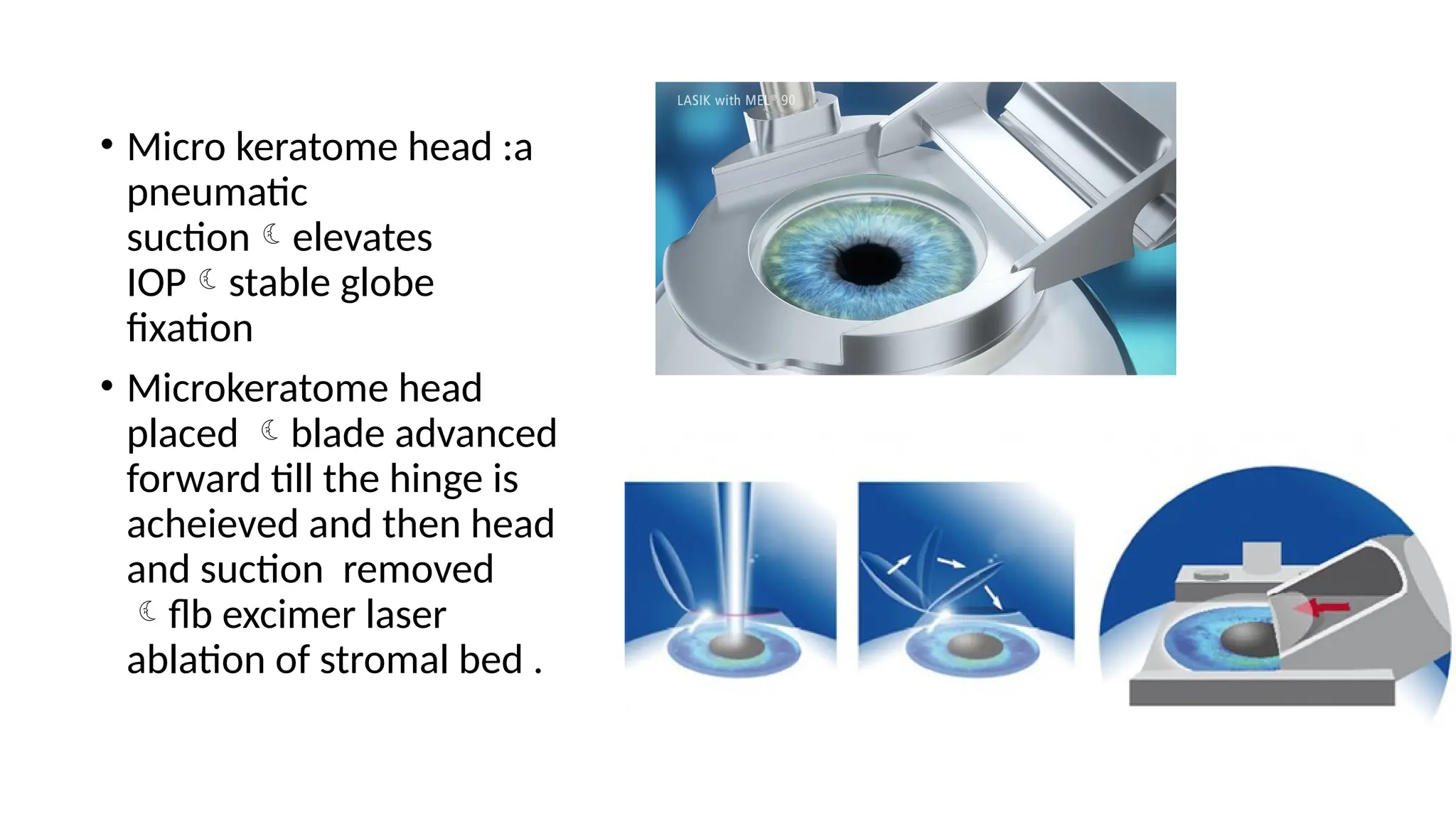
• Micro keratomehead :a
pneumatic
suctionelevates
IOPstable globe
fixation
• Microkeratome head
placed blade advanced
forward till the hinge is
acheieved and then head
and suction removed
flb excimer laser
ablation of stromal bed .
48.
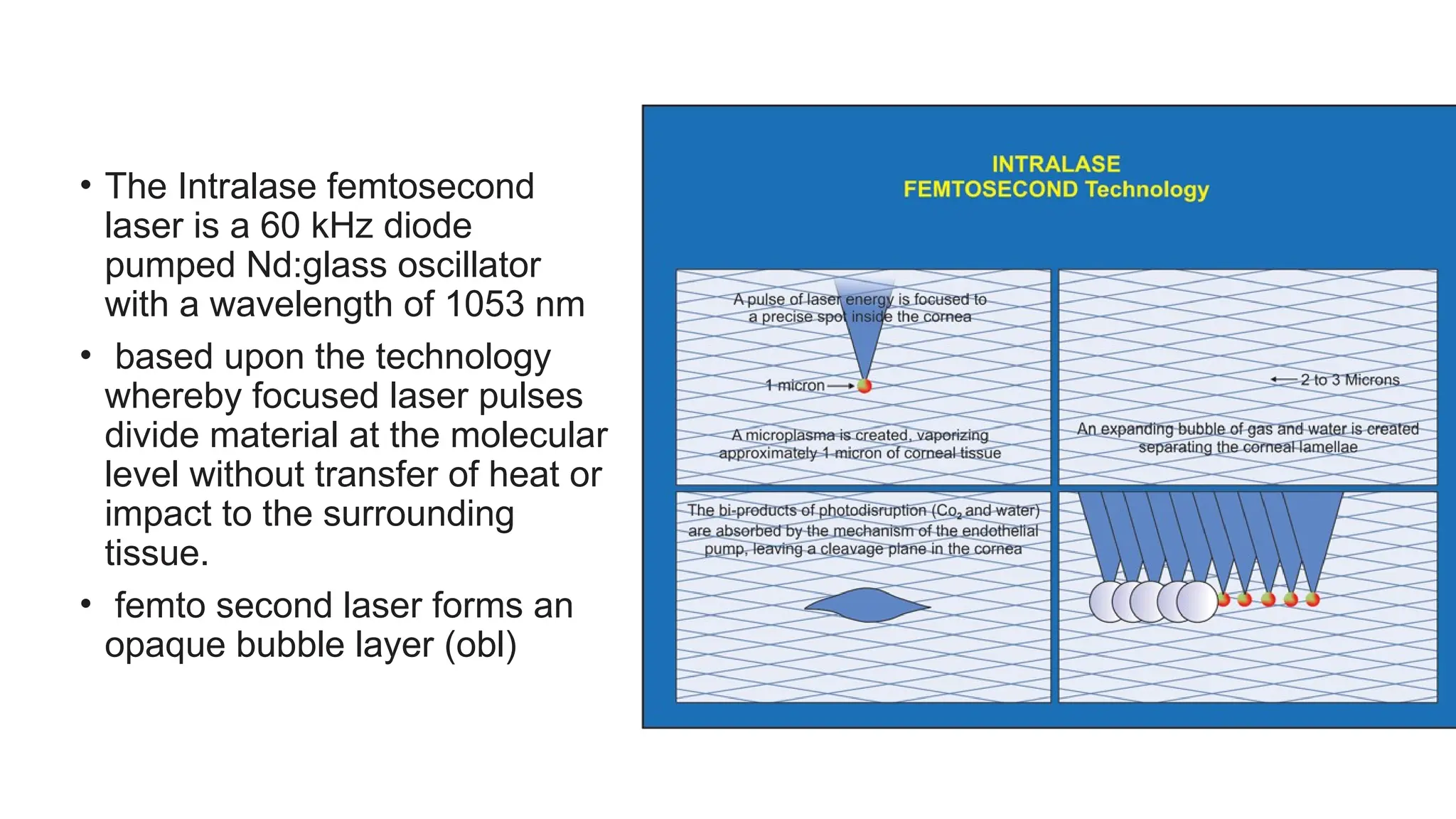
• The Intralasefemtosecond
laser is a 60 kHz diode
pumped Nd:glass oscillator
with a wavelength of 1053 nm
• based upon the technology
whereby focused laser pulses
divide material at the molecular
level without transfer of heat or
impact to the surrounding
tissue.
• femto second laser forms an
opaque bubble layer (obl)
49.
• OBL :collection of gas bubbles in
the intralamellar spaces of
cornea
• Clears spontaneously.
• Nature of OBL FORMATION
1. HIGHER energy large
cavitation bubbles rather
vapoursing heat will be
transferred to the existing
cavitation bubble increasing its
size and causing thicker OBL
50.
2.Low energy Small
microplasmas bubbles
prevent easy coalescence
during expansion resulting
thick tissue bridges .
Laser settings
• Pocketparameters : <50%corneal thickness ideally 250micronsit
prevents dense OBL formation .
• Hinge parameters:
• Large hinge angle reduces stromal bed exposed
• Narrow hinge inadequate flap for fulcrum.
• Flap bed parameters:
• Raster pattern
• Centrifugal spiralin –outrwards
• Centrifugal spiralout-inwards
• Steeper side cut angle allows easier flap reposition.
57.
Complications :
• Flaprelated complications:
1. Thin or button-holed flaps
• are seen more commonly in patients with steep corneas (>46
D)
• with poor suction.
• Treatment :replacement of the flap and applying a bandage
contact lens to avoid further displacement.
• The laser procedure should be deferred till the flap heals
smoothly.
• The patient can be taken up for recutting the flap after three
months after the best spectacle corrected visual acuity
(BSCVA) is obtained.
• Alternatively, surface ablation procedures maybe performed.
58.
2. Irregular flaps
•jamming or jerky movement of the micro-
keratome
• indicate poor assembly or maintenance of the
motor system.
• Preoperative inspection and careful alignment
and insertion of the microkeratome is essential
to avoid such complications.
3.A free cap
• usually occurs in flat corneas (<41D)
• with de-centered placement of the suction
ring.
• The laser ablation should be completed, and
the flap carefully removed and replaced in
the correct orientation on the stromal bed
59.
• Laser relatedcomplications: These include decentration and irregular
astigmatism. P atients complain of poor vision and undercorrection.
Customized lasers prevent such complications and provide better quality
vision.
• Postoperative complications: include displaced or dislocated flaps.
• Careful alignment of the flap edge should be done and slit lamp examination
performed before the patient is sent home after the laser procedure.
• If any displacement is noted, the flap should be immediately re- positioned and
smoothened out in the correct orientation.
• The patient is asked not to rub the eyes at all in the immediate postoperative
period
60.
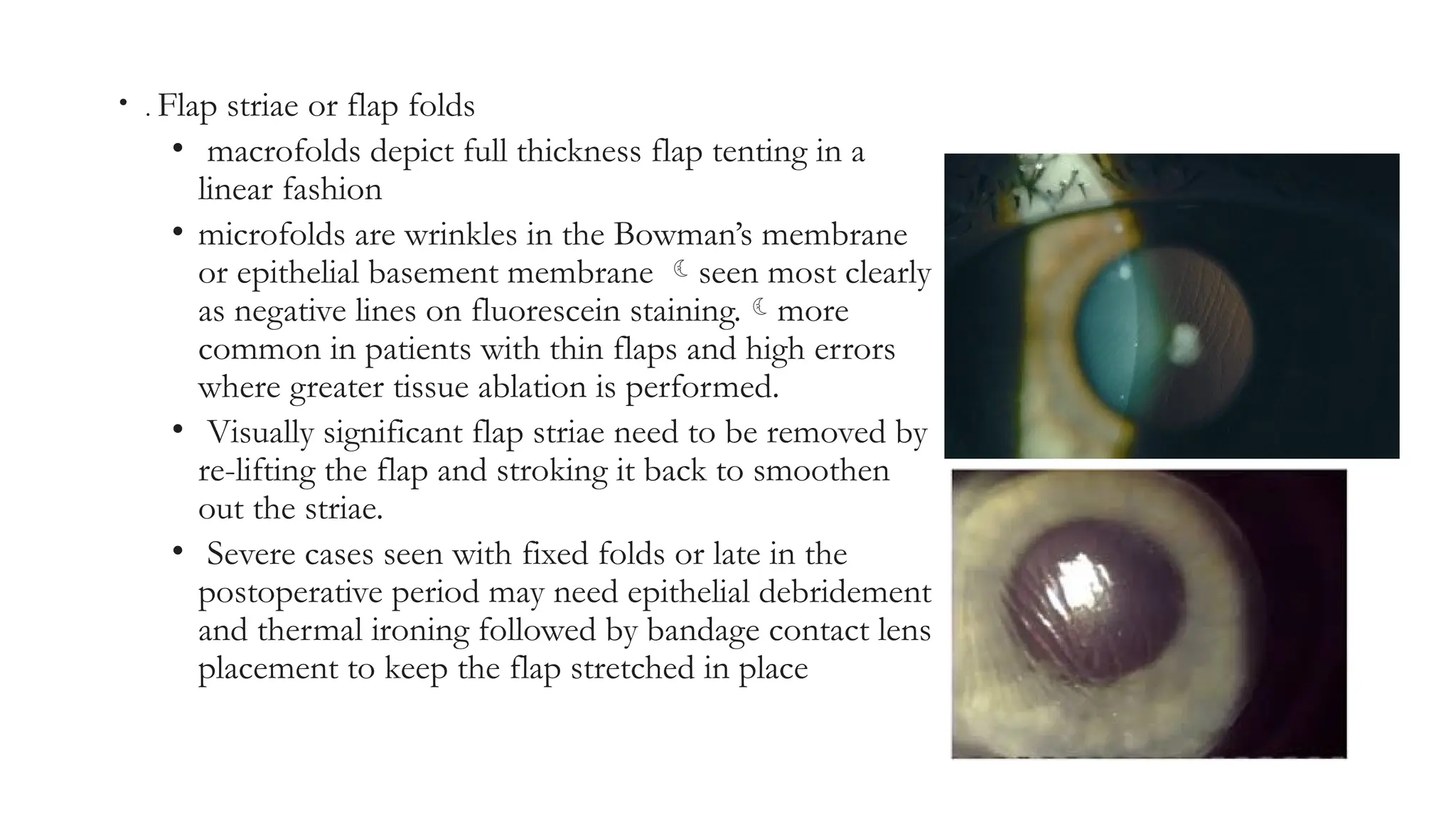
• . Flapstriae or flap folds
• macrofolds depict full thickness flap tenting in a
linear fashion
• microfolds are wrinkles in the Bowman’s membrane
or epithelial basement membrane seen most clearly
as negative lines on fluorescein staining.more
common in patients with thin flaps and high errors
where greater tissue ablation is performed.
• Visually significant flap striae need to be removed by
re-lifting the flap and stroking it back to smoothen
out the striae.
• Severe cases seen with fixed folds or late in the
postoperative period may need epithelial debridement
and thermal ironing followed by bandage contact lens
placement to keep the flap stretched in place
61.
• Epithelial ingrowth:RARE
• Treatment involves early identification and removal of the epithelial cells.
Scraping both the stromal bed and the undersurface of the flap is
essential to prevent recurrence.
62.
• 5. Diffuselamellar keratitis: Also known as
the sands of Sahara, diffuse lamellar
keratitis is a sterile inflammatory reaction
• etiology :
• unknown but is believed to be caused by
foreign cells introduced at the time of
surgery. gram-negative bacterial
endotoxinsresidue from the
microkeratome head, glove powder etc.
• C/F :pain, blurred vision, foreign body
sensation , light sensitivity and occurs
usually one to six days after
surgery ,months to years later as well.
63.
• Grade I:
•This is mild keratitis localized at the
periphery
• with minimal to no symptoms.
• Treatment:topical steroids (prednisolone
1–2 hourly)
• Grade II:
• Moderate infiltrates extend to the central
cornea
• decreased vision and photophobia
occur.
• Treatment : topical steroids +oral
steroids .
64.
• Grade III:
•Clumping of inflammatory
cells which obscure the iris
details and central infiltrates
• significant decrease in vision
is seen.
• Treatment :topical and oral
steroids
• lifting the flap to brush the
stromal bed +flap underface
and irrigation to remove all
the inflammatory cells and
debris is important to
prevent permanent damage.
65.
• Grade IV:
•Dense white central infiltrates maybe
associated with corneal melting
• loss of vision.
• The flap should be immediately lifted
to scrape and remove all the interface
debris and irrigated thoroughly.
• The infiltrate should be cultured to
rule out an infective agent.
• A drop of steroid may be placed on
the stromal bed to prevent further
inflammation
67.
• Infectiouskeratitis:Thoughinfectiouskeratitisafterlaser surgeryis rare,
• Ectasia:
• Thinningandbulgingofthecorneamayoccur due to biomechanical
weakening of the corneal tissue following laser ablation.
• Patients with preoperative abnormal topography, missed keratoconus
forme fruste cases missed .
• Corneal cross linking with riboflavin 0.1 percent and ultraviolet radiation
helps to increase the tissue rigidity and improve the biomechanical
strength. Advanced cases may need corneal transplantation
68.
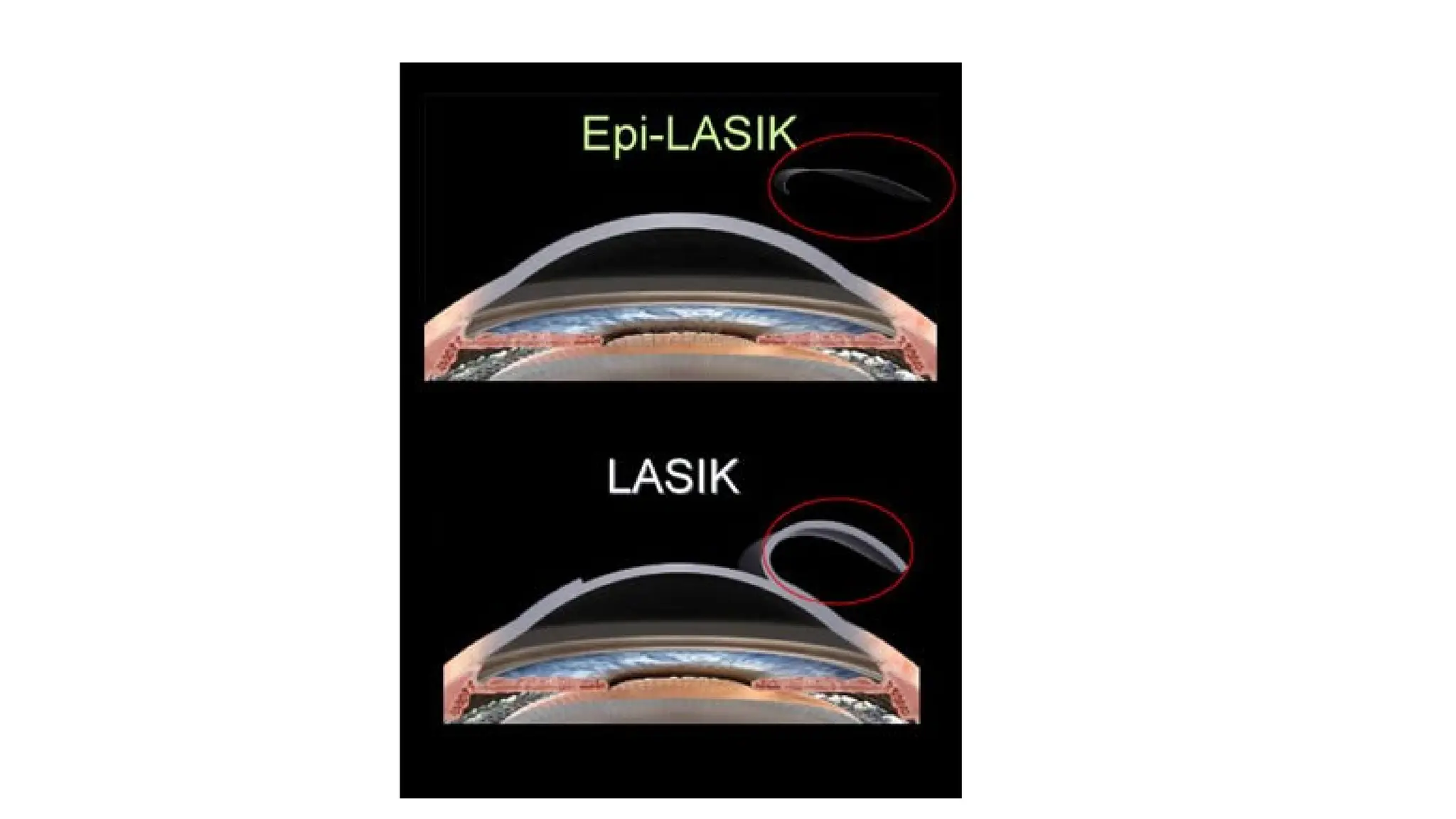
EPI-LASIK
• It usesan instrument called an epikeratome to create a flap at the level of
the basement membrane maintaining its integrity and sparing the stroma.
• It is especially useful in patients with thinner corneas.
• The excimer ablation is performed after which the thin flap may either be
reposited or removed and a bandage contact lens is placed to allow a
smoother epithelial healing
• Use of Mitomycin C drops 0.02 percent have been recommended to
reduce the chances of postoperative corneal haze.
• Retaining the epithelial flap has also been known to protect the bare
70.
SMILE
• SELECTION CRITERIA
1.Myopic correction of -10d
2. Astigmatic correction of -5D
3. Cases with mild dry eyes faster basal nerve regeneration.
4. High magnitude of refractive error minimal peripheral
collagen fibres disruption.
5. Absence of flap related complications
6. In large pupils abberations are less
71.
• c/I :
•Same as other refractive surgerirs
• Not preffered in low myopia patients thin lenticule lenticule
misdissection and cap lenticular adhesions .
72.
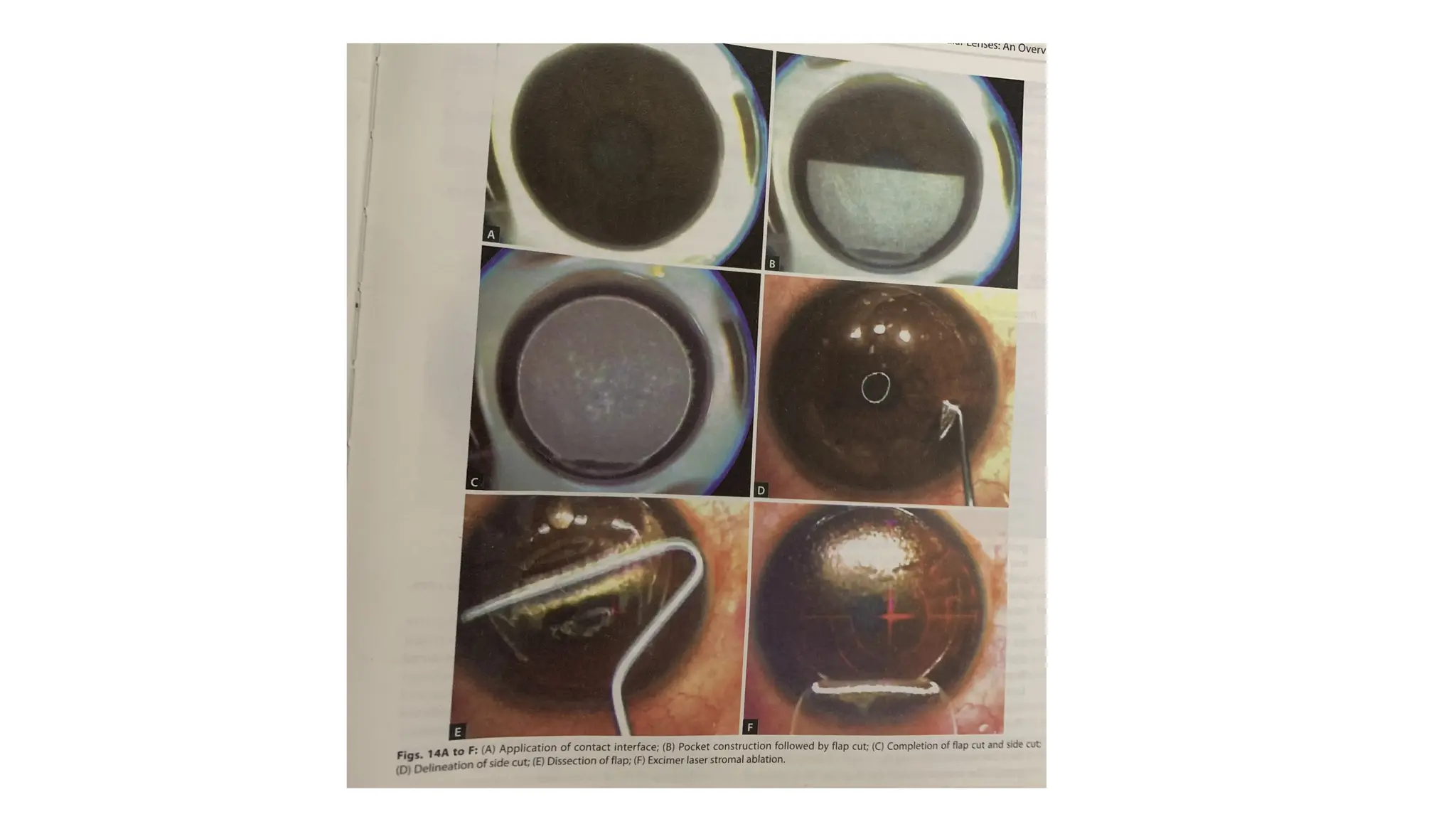
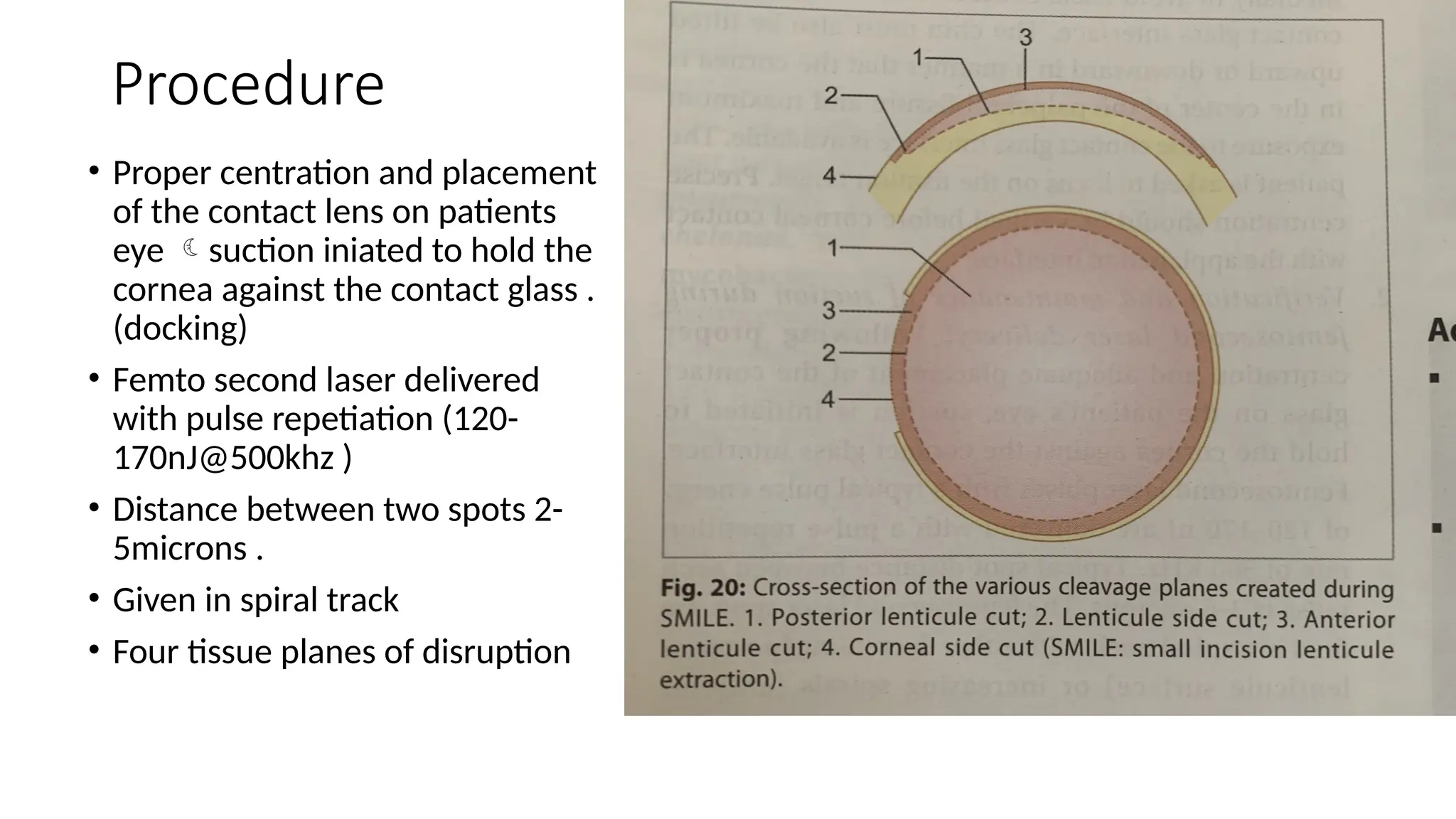
Procedure
• Proper centrationand placement
of the contact lens on patients
eye suction iniated to hold the
cornea against the contact glass .
(docking)
• Femto second laser delivered
with pulse repetiation (120-
170nJ@500khz )
• Distance between two spots 2-
5microns .
• Given in spiral track
• Four tissue planes of disruption
74.
Intracorneal Ring Segments
•Intrastromal Corneal Ring Segments
• INTACS are corneal implants which are used to change the shape of the
cornea and correct the refractive error in patients with myopia and
keratoconus.
• they consist of two, tiny clear crescent shaped pieces of PMMA which
can be inserted into the cornea .
75.
• For myopia:INTACSwork by flattening the cornea to refocus light rays
and improve vision while in keratoconus patients, INTACS flatten the
steep part of the cone and reduce vision distortions.
• They are available in various sizes which are chosen according to the
refractive error and the corneal thickness of the patient.
• A clear, central cornea with minimum corneal thickness of 450 microns
at incision site and a mesopic pupil size of less than 6 mm are preferred.
• After performing corneal topography and refraction, the size of the
INTACS and placement is planned
76.
• .
• Theincision may be made mechanically with a
diamond knife and a tunnel created by a
dissector into which the ring segments are
placed.
• Alternatively, the femtosecond laser can be
used for the same using pre programmed
parameters.
Lifting the flap by delineating
the edge
• INTACS advantages
1.central cornea undisturbed.
2. The results are rapid and predictable and if required, the INTACS can
be removed or exchanged.
3. The corneal asphericity is maintained with minimal adverse effects.
• complications :epithelial defects, channel haze, under/overcorrections,
sterile infiltrates/ epithelial cysts, infectious keratitis and ring extrusion.
79.
Phakic IOLs
• Theyare placed :
• implanted between the cornea and
lens: duophakia’ or ‘artiphakia
1. fixated in the angle enclavated to
the mid-peripheral
2. iris with a claw
3. placed in the posterior chamber
implantable contact lens .
80.
• The advantages
•Allows the crystalline lens to retain its function•
• Immediately stable, because the refractive outcome depends
less on the healing processes
• Excellent vision even in dim light conditions
• Removable and exchangeable
• Easily adjustable with complementary fine-tuning corneal
surgeries.
81.
• the idealcandidates
• >21 years old
• have had stable refraction (change in vision <0.5 D) over at least one
year
• are poor candidates for excimer laser surgery
• have poor tolerance of contact lenses or glasses
• have irido-corneal angle >30 degrees
• have central endothelial cell count >2300 cells/mm2
>2000 if >40 years
old,
• a mesopic pupil size <5-6 mm.
• high refractive errors
• thin corneas,
82.
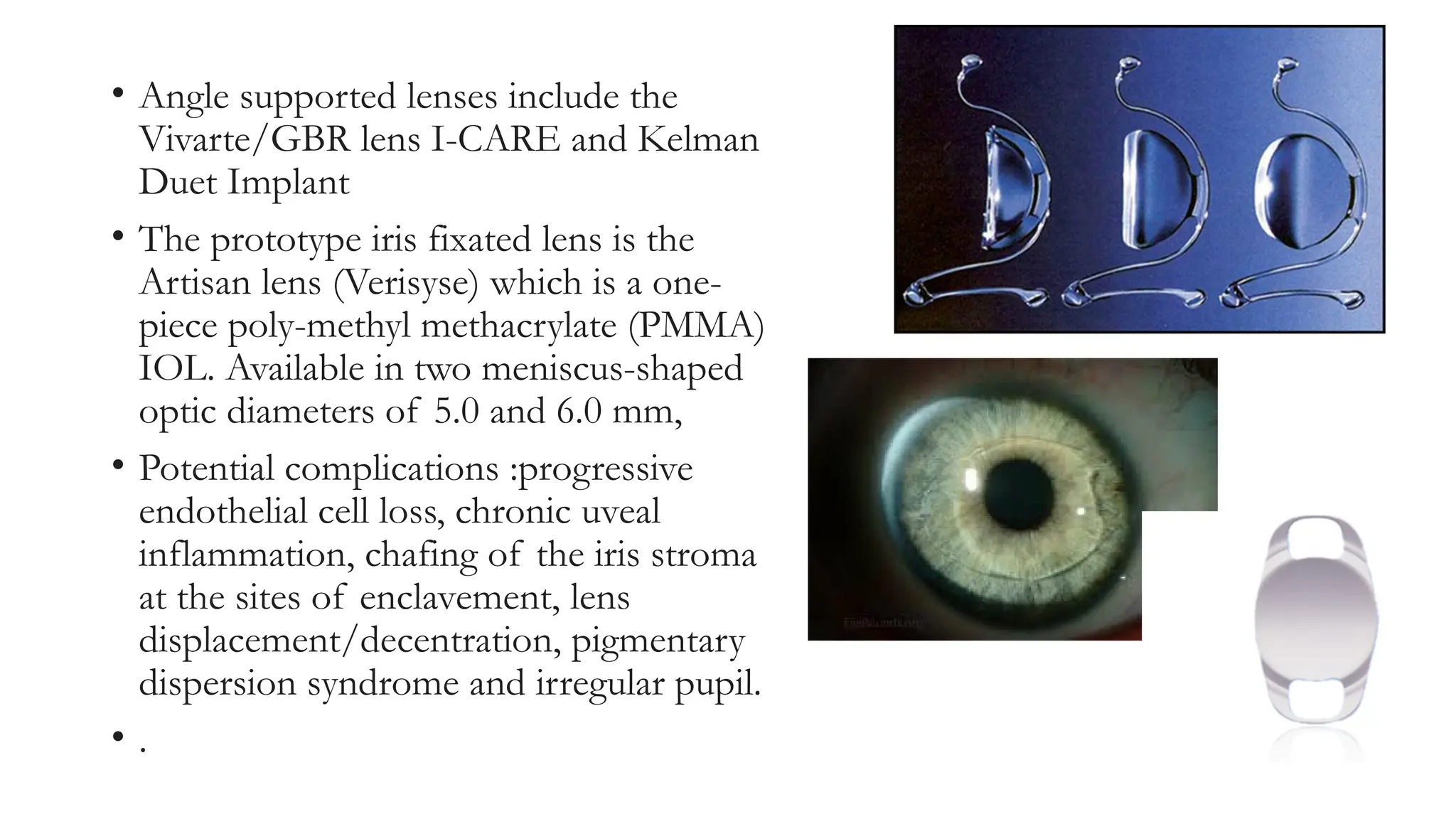
• Angle supportedlenses include the
Vivarte/GBR lens I-CARE and Kelman
Duet Implant
• The prototype iris fixated lens is the
Artisan lens (Verisyse) which is a one-
piece poly-methyl methacrylate (PMMA)
IOL. Available in two meniscus-shaped
optic diameters of 5.0 and 6.0 mm,
• Potential complications :progressive
endothelial cell loss, chronic uveal
inflammation, chafing of the iris stroma
at the sites of enclavement, lens
displacement/decentration, pigmentary
dispersion syndrome and irregular pupil.
• .
83.
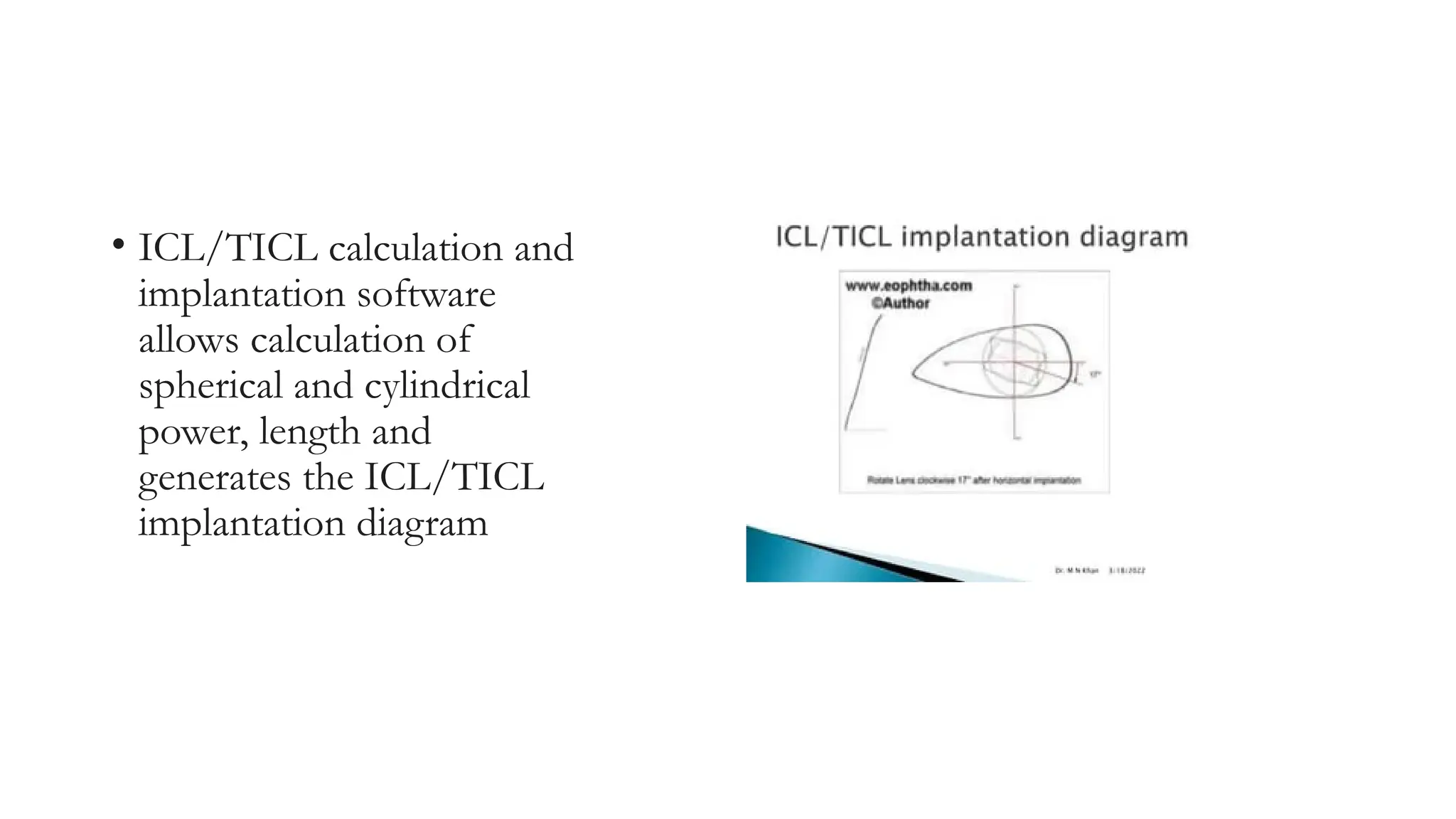
• ICL/TICL calculationand
implantation software
allows calculation of
spherical and cylindrical
power, length and
generates the ICL/TICL
implantation diagram
• ICL wasdesigned so that its haptic rest horizontally on ciliary
sulcusand the length should be equal to horzintal sulcus diameter .
• ICL
• Too short ASC increased and rotation is secondary to an unstable fixation.
• Too longover crowding at the angle angle closure glaucoma
• ACD : measured Using orbscan /penta cam
86.
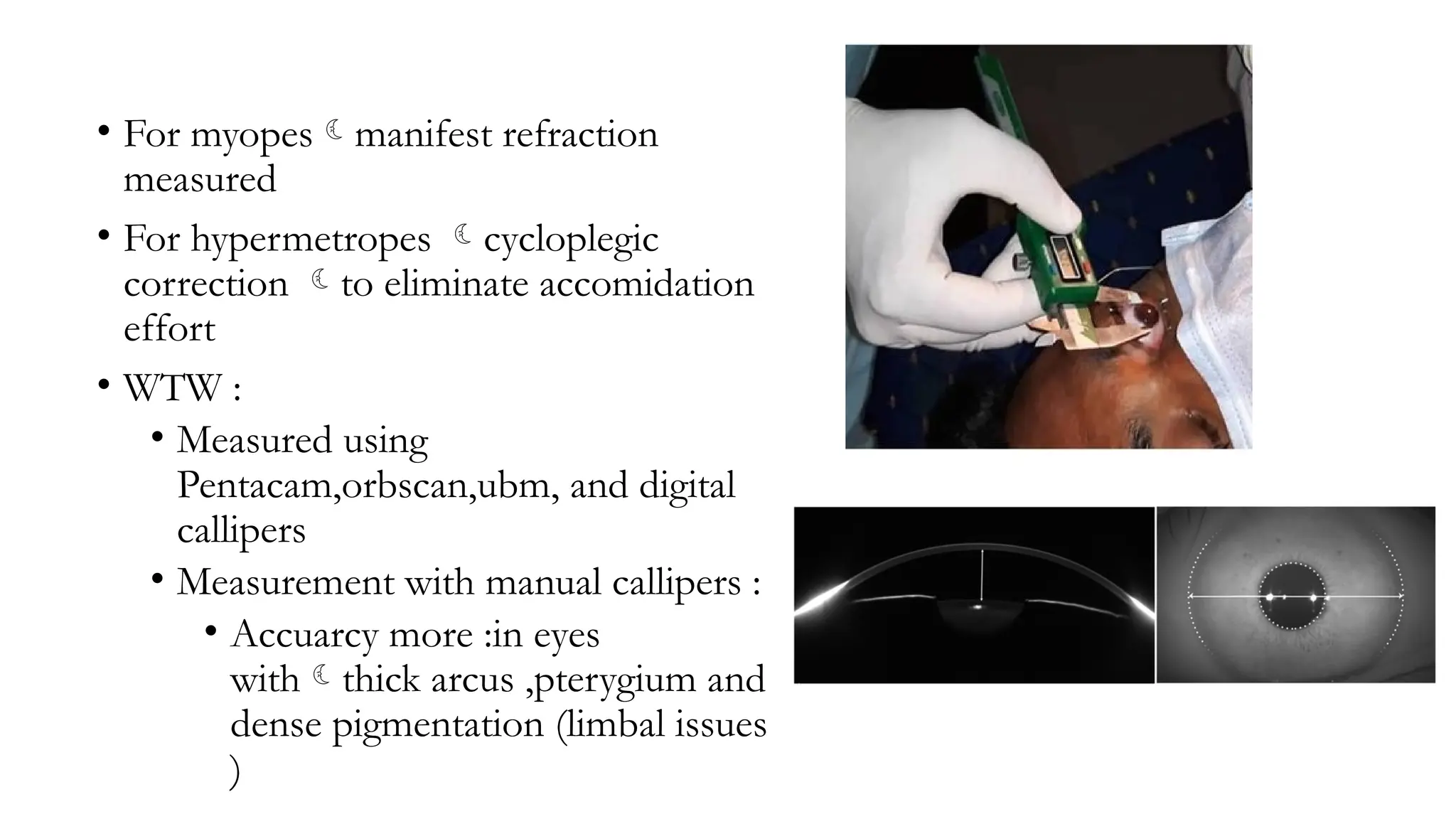
• For myopesmanifestrefraction
measured
• For hypermetropes cycloplegic
correction to eliminate accomidation
effort
• WTW :
• Measured using
Pentacam,orbscan,ubm, and digital
callipers
• Measurement with manual callipers :
• Accuarcy more :in eyes
withthick arcus ,pterygium and
dense pigmentation (limbal issues
)
87.
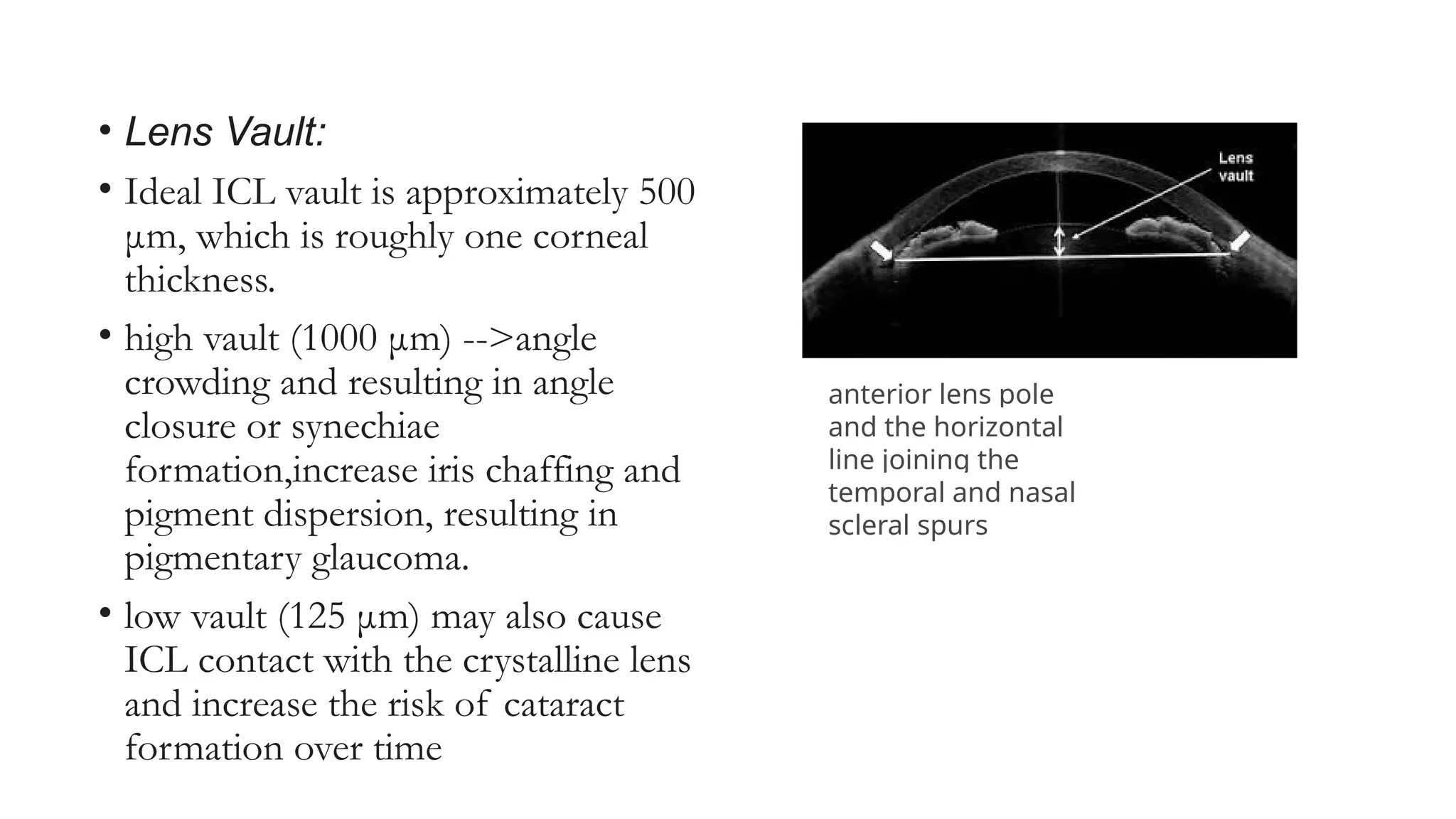
• Lens Vault:
•Ideal ICL vault is approximately 500
μm, which is roughly one corneal
thickness.
• high vault (1000 μm) -->angle
crowding and resulting in angle
closure or synechiae
formation,increase iris chaffing and
pigment dispersion, resulting in
pigmentary glaucoma.
• low vault (125 μm) may also cause
ICL contact with the crystalline lens
and increase the risk of cataract
formation over time
anterior lens pole
and the horizontal
line joining the
temporal and nasal
scleral spurs
88.
• Peripheral iridotomy
•done one to two weeks before the
surgery to provide an outlet for the
aqueous flow around the lens.
• Alternatively it may be performed
intraoperatively after ICL
implantation with a Vannas scissors
or a vitrectomy cutter.
• It should be sufficiently wide (at
least 500 m), positioned superiorly
(from 11 to 1 o’clock) and well
away from the haptics placement.
89.
• peripheral iridotomiesare strongly recommended to prevent
pupillary block for both anterior and posterior pIOLs.
• Main incisions are typically performed on the steep corneal
axis to reduce surgically induced astigmatism.
90.
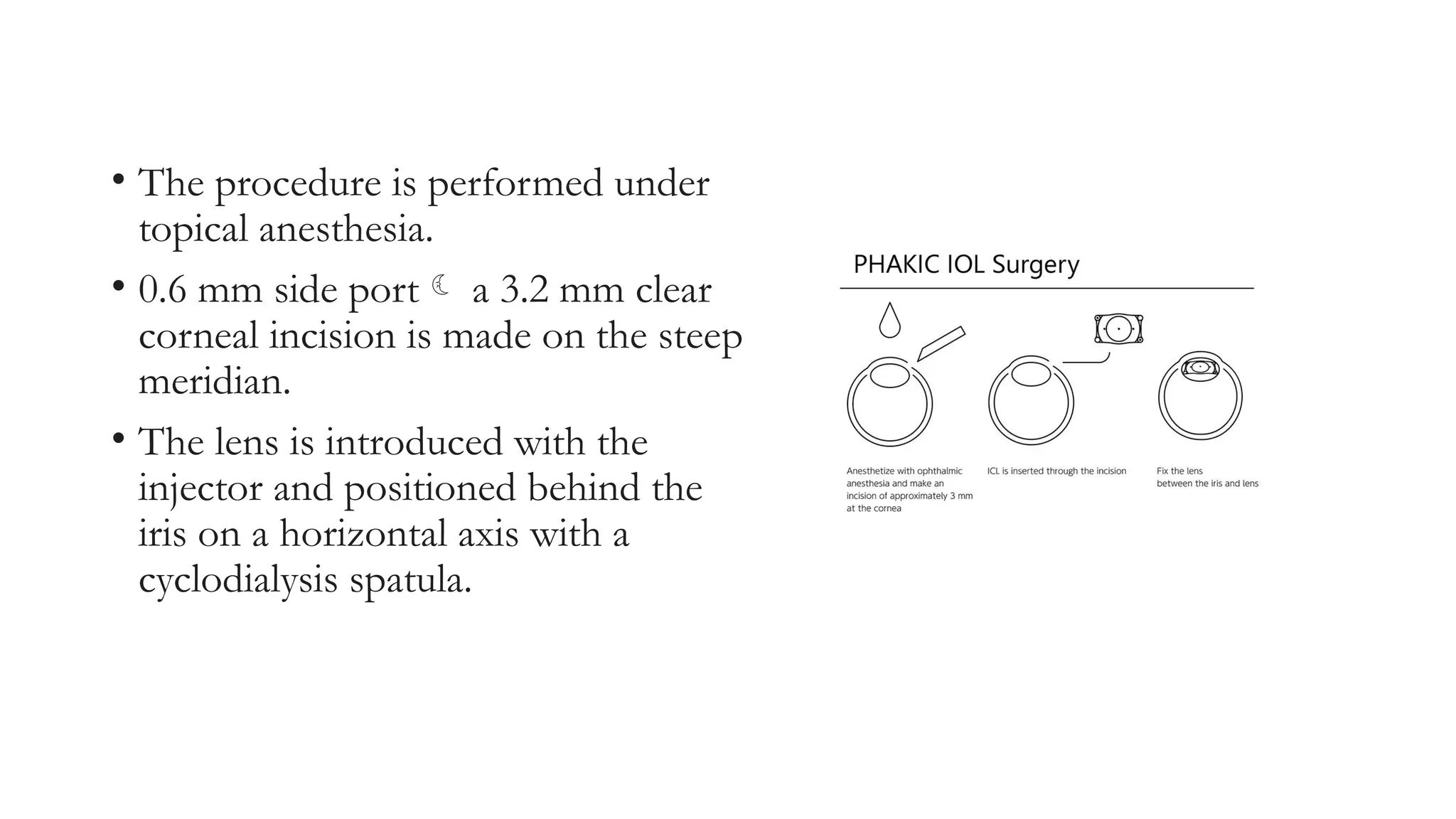
• The procedureis performed under
topical anesthesia.
• 0.6 mm side port a 3.2 mm clear
corneal incision is made on the steep
meridian.
• The lens is introduced with the
injector and positioned behind the
iris on a horizontal axis with a
cyclodialysis spatula.
91.
• To controlfor potential cyclotorsion in a supine position, the zero horizontal
axis is marked preoperatively on the slitlamp.
• The lens is implanted temporally and gently rotated to align the axis with the
cylindrical axis of the patient.
• Complete removal of viscoelastic material is essential.
• Presence of residual viscoelastic material behind the implant may cause
opacification of the crystalline lens.
• A miotic agent is injected and the aspiration is completed. The incision is
closed by hydrating the corneal incision.
•
92.
• contraindication
1. activeanterior segment disease
2. recurrent or chronic uveitis
3. cataracts, previous ocular surgery
4. glaucoma or IOP >21mmHg
5. preexisting macular pathology, retinal disease, anomalous
irises or pupils.
BIOPTICS
• For eyeswith large refractive errors, one refractive procedure alone may not
be sufficient to correct the entire refractive error.
• Combining two or three procedures together is called bioptics or trioptics
respectively.
• Lenticular options are available in the form of phakic IOls, toric IOLs and
piggyback IOLs
• corneal options for bioptics include corneal relaxing incisions (CRIs),
anterior limbal relaxing incisions (ALRI), laser-assisted epithelial
keratomileusis (LASEK), photore- fractive keratectomy (PRK), conductive
keratoplasty (CK) and intrastromal ring implants.
95.
Presbyopia treatment
1. Themost widely used standard
protocol has been the use of
progressively hyperopic spectacles
which take over the near focus of
the crystalline lens.
2. Monovision correction (using
contact lenses/monofocal
intraocular lenses)
3. Multifocal IOLs
4. Accommodative IOLs
5. Phakic multifocal IOL
.
• Monovision correction:
•correcting one eye for distance and the other eye for near so that the
patient is able to perform all activities at near and far distance without
the aid of glasses.
• Ideally the dominant eye is corrected for distance vision and the non-
dominant eye for near vision.82
• Monovision maybe obtained using contact lenses, monofocal IOLs,
LASIK or in combination with CK.
CK- Conductive keratoplasty
•The principle of Conductive
keratoplasty (CK)) is based on that
of thermokeratoplasty, using
radiofrequency (RF) energy to
reshape the cornea and modify its
refractive characteristics.
• CK may be performed for low to
moderate hyperopia (between +0.75
and +3.00 diopters).
100.
• To performthe procedure, a
handpiece with a KeratoplastTM Tip
delivers controlled RF energy
directly to the corneal stroma in a
ring pattern.
• Conductive keratoplasty creates a
purse-string effect that steepens the
central cornea through a ring of
application spots around the
periphery of the cornea.
101.
Anterior Ciliary Sclerotomy(ACS):
• Multiple incisions are made in the sclera over the
ciliary muscle to increase the distance between
the lens equator and the ciliary muscle.
• While some studies have shown minor
improvements in presbyopic vision, others found
no improvement, but concluded that this
procedure weakens the sclera significantly so that
it may rupture more easily.
102.
• Laser presbyopiareversal (LAPR): This is similar to ACS, but uses laser
instead of surgical knife.
• The laser vaporizes the tissue in eight radial lines on the sclera.
• This removal of tissue thins the sclera and increases the amount of space
for the ciliary muscle beneath it.
103.
• Surgical reversalof presbyopia (SRP) with scleral expansion bands: The effect of
the scleral expansion band is based on the theory of Schachar that states
that the crystalline lens is under increased equatorial zonular tension
during accommodation.
• Now a separate PMMA segment is placed in each of the 4 oblique
quadrants of the eye.
• The overall response has been favorable with no change in distance
refraction, best corrected visual acuity, or axial length.
• Common adverse effects include subconjunctival hemorrhage, transient
astigmatism, fluctuating near vision, and dry eyes which usually resolve in
six to eight weeks.
104.
• Safety concernsabout the procedure include the possibility of infection,
degradation of the implants over time, and compromised blood
circulation in the eye.
105.
• Corneal inlays:
•Corneal inlays are five to ten microns thick intracorneal implants with a
diameter of 3.8 mm and a central aperture of 1.6 mm.
• Made of polyvinylidene fluoride material, they increase the depth of
focus by blocking out unfocussed light.