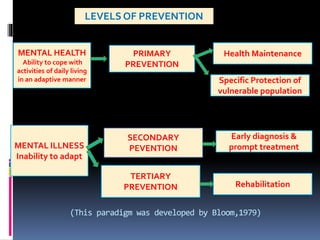
The document elaborates on preventive psychiatry introduced by Gerald Caplan in 1964, outlining three levels of prevention: primary, secondary, and tertiary. Primary prevention aims to reduce the incidence of mental disorders through individual and environmental strategies; secondary prevention focuses on early symptom recognition and treatment; and tertiary prevention targets individuals with existing mental illnesses to minimize disability and promote rehabilitation. The roles of nurses in each prevention level include providing education, support, and rehabilitation services to both individuals and families.

![DEFINITION
Rehabilitation is " an attempt to provide the
best possible community role which will
enable the patient to achieve the maximum
range of activity, interest and of which he is
capable". -Maxwell Jones [1952]](https://image.slidesharecdn.com/preventivepsychiatric-200817063929/85/Preventive-psychiatric-27-320.jpg)