Downloaded 622 times




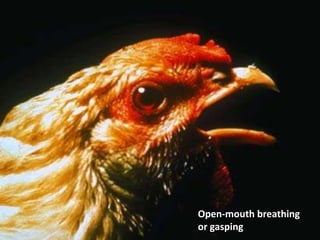



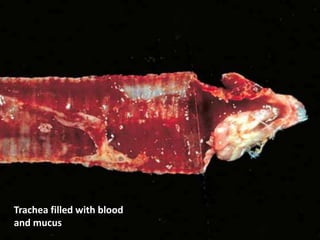


This document provides an overview of Infectious Laryngotracheitis (ILT), a viral respiratory infection of chickens. It discusses the etiology (caused by Gallid herpesvirus 1), epidemiology (spread through direct contact with infected birds), clinical signs (gasping, coughing, nasal discharge), diagnosis (post-mortem lesions include exudate in the trachea), and prevention/control (vaccination and strict biosecurity to limit virus spread and mixing of infected and susceptible birds).











































































































