Downloaded 1,238 times










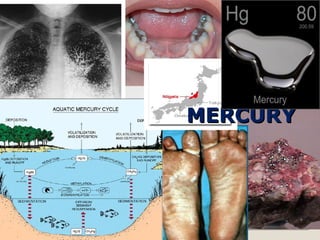



























Toxic metals are harmful substances with no biological role, leading to significant health issues as they interfere with metabolic processes in humans. Current industrial practices and waste management have exposed the population to unprecedented levels of toxic metals such as lead, mercury, and arsenic. Management of toxicity involves specific chelating agents and varying treatment protocols based on the type and severity of exposure.