
Download as PDF, PPTX
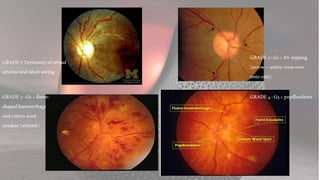

Hypertensive retinopathy is characterized by changes in the retinal fundus due to systemic hypertension, with grading based on severity and clinical features. Pathogenesis involves vasoconstriction, atherosclerosis, and increased vascular permeability, with management primarily focusing on controlling blood pressure to prevent progression. While chronic cases rarely lead to vision loss, malignant cases require careful treatment to avoid severe complications.































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








