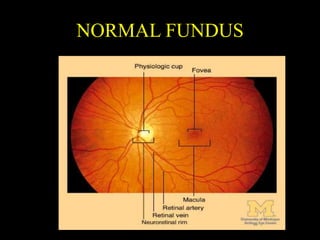
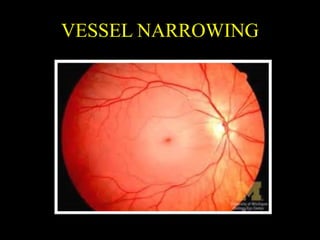
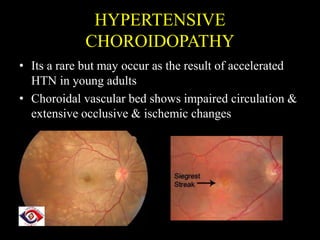
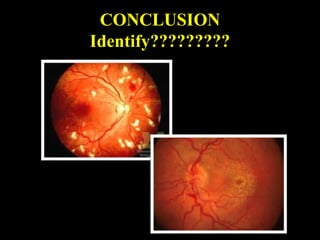
This document discusses hypertension (high blood pressure) and its effects on the eyes. It defines normal and high blood pressure and classifies hypertension based on cause and severity. It describes potential causes of hypertension and symptoms someone may experience. Complications of uncontrolled hypertension include damage to organs like the heart, brain, kidneys and eyes. The document focuses on three eye conditions caused by hypertension: hypertensive retinopathy, characterized by changes to retinal blood vessels; hypertensive choroidopathy, involving the choroidal blood vessels; and hypertensive optic neuropathy related to swelling of the optic nerve. Each condition is described in detail with examples of associated fundus findings.