Hypertensive retinopathy is caused by chronically elevated blood pressure and progresses through vasoconstrictive, sclerotic, and exudative phases. It is diagnosed through fundus examination showing arteriolar narrowing, arteriovenous nicking, hemorrhages, exudates and other changes. The severity is classified using systems like Keith-Wagener-Barker or Wong-Mitchell, with more severe grades indicating complications like papilledema. Differentiating it from similar conditions like diabetic retinopathy requires considering the medical history of hypertension versus other risk factors.


![ The arteriosclerotic changes in hypertensive retinopathy are caused by chronically
elevated blood pressure (BP)
Elevated blood pressure defined as SBP >140 mmHg and DBP >90 mmHg.[1]
Can be caused by either chronic primary or secondary hypertension (e.g.
pheochromocytoma, primary hyperaldosteronism, Cushing’s syndrome, renal parenchymal
disease, renal vascular disease, coarctation of the aorta, obstructive sleep apnea,
hyperparathyroidism, and hyperthyroidism).[2]
ETIOLOGY
1. American Academy of Ophthalmology. Basic and Clinical Sciences Course (Lifelong Education for the Ophthalmologist). San Fransisco. 2006.
2. Katakam, R., Brukamp, K., and Townsend, R.R. What is the proper workup of a patient with hypertension? Cleve Clin J Med. 2008;75:663-72.](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-2-320.jpg)
![EPIDEMIOLOGY
Erden et al. showed that the incidence of hypertensive retinopathy directly proportional to
the severity and duration of hypertension[1]
A study in German population, the incidence of hypertensive retinopathy was 10.7% (from
12,751 persons) with a median follow-up time of 8.6 years[2]
A study in DR. M. Djamil Hospital, Padang, Indonesia, found that hypertensive retinopathy
was present in 66.67% hypertensive patients[3]
Chronic kidney disease (CKD) was found to be the most significant factor to predict severe
hypertensive retinopathy[4]
1. Erden S, Bicakci E. Hypertensive retinopathy: incidence, risk factors, and comorbidities. Clin Exp Hypertens. 2012;34(6):397-401
2. Alexander Karl-Georg Schuster, Stella Hoh, Karl Neubert, Ahmad Haj Ibrahim, Stefan Nickels, Christina A. Korb, Andreas Schulz, Thomas Muenzel, Matthias Michal, Irene Schmidtmann, Karl Lackner, Philipp Wild,
Norbert Pfeiffer; Prevalence of hypertensive retinopathy and its risk for mortality – results from the Gutenberg Health Study. Invest. Ophthalmol. Vis. Sci. 2020;61(7):1308.
3. Rahman K, Yusticia RY. Profil Retinopathy Hipertensi di Rumah Sakit Dr. M Djamil Padang. J Kesehat Andalas. 2018;7(Supplement 1):19. .
4. Kabedi NN, Mwanza JC, Lepira FB, Kayembe TK, Kayembe DL. Hypertensive retinopathy and its association with cardiovascular, renal and cerebrovascular morbidity in Congolese patients. Cardiovasc J Afr. 2014
Sep-Oct;25(5):228-32.](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-3-320.jpg)
![PATOPHYSIOLOGY
Retinal blood vessels have distinct features that differentiate them from other blood vessels, including:[1]
1. The absence of sympathetic nerve supply
2. Local autoregulation of blood flow
3. Presence of blood-retinal barrier
An increase in systemic BP is transferred directly to the to the vessels which initially constrict.
A further increase in BP overcomes this compensatory tone and damage to the muscle layer and endothelium
ensues.
Blood pressure elevation continues
Hypertensive retinopathy goes through 3 phases: vasoconstrictive, sclerotic, and exudative phases[2]
1. Chaine G, Kohner EM. [Hypertensive retinopathy]. J Fr Ophtalmol. 1983;6(12):995-1005.
2. Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 22 February 2022]. Available on: https://www.ncbi.nlm.nih.gov/books/NBK525980/](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-4-320.jpg)
![3 PHASES OF HYPERTENSIVE RETINOPATHY
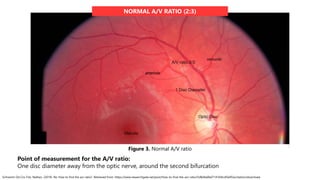
Vasoconstrictive Phase
The local autoregulatory mechanisms
come into play
This autoregulatory mechanisms cause
vasospasm and retinal arteriole
narrowing, which is evident by the
decrease in the arteriole to venule ratio
(Normal = 2:3).
Sclerotic Phase
Persistent elevated BP cause
changes in vessel wall
These changes include:
Thickening of the intimal layer
Hyperplasia of the media layer
Hyaline degeneration of the
arteriolar wall
Exudative Phase
Disruption of the blood-brain barrier
and leakage of plasma and blood
into the vessel wall
Typically seen in severely increased
BP patients
Leakage of plasma and blood into
the vessel wall cause disruption in
the local autoregulatory mechanism
Causing retinal hemorrhages (flame-shaped and
dot blot), hard exudates, retinal ischemia (cotton-
wool spots), and necrosis of smooth muscle.
Leads to a severe form of arteriolar narrowing,
arteriovenous (AV) crossing changes, and
widening and accentuation of light reflex
(silver and copper wiring)
Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 22 February 2022]. Available on: https://www.ncbi.nlm.nih.gov/books/NBK525980/](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-5-320.jpg)
![DIAGNOSIS
Diagnosis based upon its clinical appearance on dilated fundoscopic exam and coexistent hypertension[1,2]
HISTORY OF
HYPERTENSION
Focus on disease history, symptoms of hypertension, and its complications
Most patients are asymptomatic
Symptoms: headaches*, eye pain*, reduced visual acuity*, focal neurological deficits, chest pain,
shortness of breath, dyspnea on exertion, paroxysmal nocturnal dyspnea, orthopnea, and
palpitation
Complications: history of stroke/transient ischemic attack, coronary or peripheral vascular disease,
and heart failure
PHYSICAL
EXAMINATION
Focus on vital signs (especially blood pressure) and dilated fundoscopy
Fundus exam is necessary for staging of hypertensive retinopathy
1. Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 22 February 2022]. Available on: https://www.ncbi.nlm.nih.gov/books/NBK525980/
2. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022]. Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis
*Symptoms of acute malignant hypertension](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-6-320.jpg)
![FUNDOSCOPIC FEATURES
AV crossing changes[1]
Salus’s sign: retinal vein deflection as it crosses the arteriole
Gunn’s sign: retinal vein tapering on either side of the AV crossing
Bonnet’s sign: banking of retinal vein distal to the AV crossing
1. Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 22 February 2022]. Available on: https://www.ncbi.nlm.nih.gov/books/NBK525980/
2. Epomedicine. Hypertensive Retinopathy Grading – Simplified [Internet]. Epomedicine; 2019 Jun 1 [cited 2022 Feb 19]. Available from: https://epomedicine.com/medical-students/hypertensive-retinopathy-grading-simplified/.
Figure 1. AV crossing changes[2]](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-7-320.jpg)
![Arterial Changes[1]
Decrease in AV ratio to 1:3 (normal ratio 2:3)
Change in the arteriolar light reflex (copper
and/or silver wiring)
Figure 2. Copper-wiring, arteriovenous nicking and silver-wiring
seen in a patient with hypertensive retinopathy[2]
1. Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 22 February 2022]. Available on: https://www.ncbi.nlm.nih.gov/books/NBK525980/
2. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022]. Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-8-320.jpg)
![ARTERIOLE
DECREASED A/V RATIO (1:3)
VENULE
Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 24 February 2022]. Available on: https://www.statpearls.com/ArticleLibrary/viewarticle/35600
Figure 4. Decreased A/V ratio](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-10-320.jpg)
![Retinal Changes[1]
Retinal hemorrhages
Dot-blot hemorrhages
Bleeding in the inner retinal layer
Flame shaped hemorrhage
Bleeding in the superficial retinal layer
Retinal exudates
Hard exudate
Lipid deposits in the retina
Soft exudate
Ischemia of the nerve fibers (cotton wool
spots)
Figure 5. AV crossing changes, macular star, and cotton wool
spots[2]
1. Modi, P., Arsiwalla, T. Hypertensive retinopathy [Internet]. StatPearls Publishing. 2021 [Accessed on 22 February 2022]. Available on: https://www.ncbi.nlm.nih.gov/books/NBK525980/
2. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022]. Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis
Macular Changes[1]
Formation of macular star due to deposition of hard
exudates around the macula.](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-11-320.jpg)
![Figure 6. Features of hypertensive retinopathy[2]
1. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022]. Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis
2. Kulenkamp, E. Hypertensive retinopathy [Internet]. Available on: http://morancore.utah.edu/basic-ophthalmology-review/hypertensive-retinopathy/
Optic Nerve Changes[1]
Hypertension may lead to optic
neuropathy (specifically presents as optic
disk swelling)
Signs of optic neuropathy are:
1. Flame shaped hemorrhage at the disc
margin
2. Blurred disc margin
3. Congested retinal vein
4. Papilledema
5. Secondary macular exudates](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-12-320.jpg)
![MODIFIED SCHEIE CLASSIFICATION OF HYPERTENSIVE RETINOPATHY[1]
1. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022]. Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis
2. Epomedicine. Hypertensive Retinopathy Grading – Simplified [Internet]. Epomedicine; 2019 Jun 1 [cited 2022 Feb 19]. Available from: https://epomedicine.com/medical-students/hypertensive-retinopathy-grading-simplified/.
Grade 0: No changes
Grade 1: Barely detectable arterial narrowing
Grade 2: Obvious arterial narrowing with focal irregularities
Grade 3: Grade 2 + retinal hemorrhages, exudates, cotton wool spots, or retinal edema
Grade 4: Grade 3 + papilledema
Figure 7. Grade 3-4 of hypertensive retinopathy[2]](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-13-320.jpg)
![MODIFIED SCHEIE CLASSIFICATION
OF HYPERTENSIVE RETINOPATHY
Walsh JB et al. Chapter 13: Systemic Hypertension and the Eye. [Internet]. 2022. Available from:
http://www.oculist.net/downaton502/prof/ebook/duanes/pages/v3/v3c013.html
A. Grade I narrowing of the arterioles
B. Grade II: generalized narrowing,
focal constriction, arteriolar sclerosis
with widening of the reflex stripe.
C. Grade III: generalized narrowing,
focal constriction, hemorrhages, and
exudate, arteriolar sclerosis with
widening of the light reflex.
D. Grade IV: generalized narrowing,
focal constriction, hemorrhages, and
exudates and edema of the disc with
arteriolar sclerosis.
Figure 8. Funduscopic findings based on Modified Scheie Classification[2]](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-14-320.jpg)
![KEITH-WAGENER-BARKER CLASSIFICATION[1]
A. Grade 1:
Mild, generalized constriction of retinal arterioles
B. Grade 2:
Definite focal narrowing of retinal arterioles + AV
nicking (arrows)
C. Grade 3:
Grade 2 + flame-shaped hemorrhages + cotton-
wool spots + hard exudates
D. Grade 4:
Severe Grade 3 retinopathy + papilledema or
retinal edema
Figure 9. Funduscopic findings based on Keith-Wagener-Barker Classification[2]
1. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022].
Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis
2. Anonymous. Hypertensive retinopathy [Internet]. [Accessed on 24 February 2022]. Available on:
https://basicmedicalkey.com/hypertensive-retinopathy-2/](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-15-320.jpg)
![WONG AND MITCHELL CLASSIFICATION OF HYPERTENSIVE RETINOPATHY
1. Wong TY, Mitchell P. Hypertensive retinopathy. N Engl J Med. 2004;351:2310–2317. doi:10.1056/NEJMra032865
2. Aissopou EK, Papathanassiou M, Nasothimiou EG, Konstantonis GD, Tentolouris N, Theodossiadis PG, Papaioannou TG, Sfikakis PP, Protogerou AD. The Keith-Wagener-Barker and Mitchell-Wong grading systems for hypertensive
retinopathy: association with target organ damage in individuals below 55 years. J Hypertens. 2015 Nov;33(11):2303-9. doi: 10.1097/HJH.0000000000000702. PMID: 26335430.
Mitchell-Wong seems preferable to the Keith-Wagener-Barker classification system, for reasons of simplifying
clinical practice and the grades of retinopathy were more strongly associated with systemic issues[1,2]](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-16-320.jpg)
![DIFFERENTIAL DIAGNOSIS
Conditions that have similar features with hypertensive retinopathy includes most notably diabetic
retinopathy, radiation retinopathy, and retinal vein occlusion[1]
CLINICAL FINDINGS HYPERTENSIVE RETINOPATHY DIABETIC RETINOPATHY RADIATION RETINOPATHY
History History of hypertension History of diabetes
History of radiation
(e.g. nasopharyngeal carcinoma
treatment)[2,3]
Funduscopic Findings
AV changes
Arterial changes
Retinal changes
Macular changes
Optic nerve changes
Similar findings with
hypertensive retinopathy
Similar findings with
hypertensive retinopathy
Optic disc edema can also be found in diabetic papillopathy, anterior ischemic optic neuropathy, and
neuroretinitis[1]
1. American Academy of Ophthalmology. Hypertensive retinopathy [Internet]. 2021 [Accessed on 22 February 2022]. Available on: https://eyewiki.aao.org/Hypertensive_Retinopathy#Diagnosis
2. Ho, IV. Radiation retinopathy [Internet]. 2012 [Accessed on 24 February 2022]. Available on: http://www.retina.com.au/case-of-the-monthdec-2012/
3. Raja V, Rajagopalan S, Kashab T, Moriarty B. Radiation retinopathy: a mistaken diagnosis of hypertensive retinopathy. Clinical and Experimental Optometry. 2007;90(6):468-470.](https://image.slidesharecdn.com/hypertensiveretinopathy2-230621022107-45845488/85/Hypertensive-Retinopathy-2-pptx-17-320.jpg)




































































