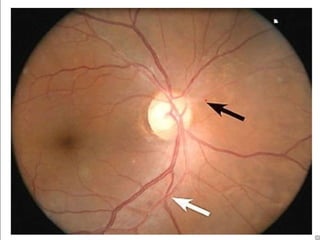
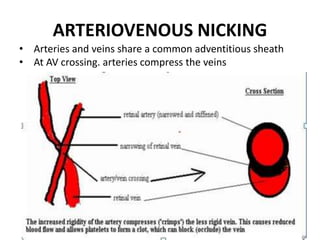
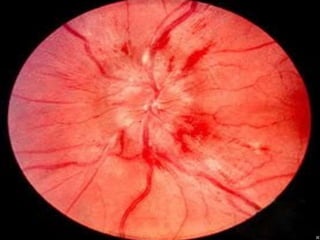
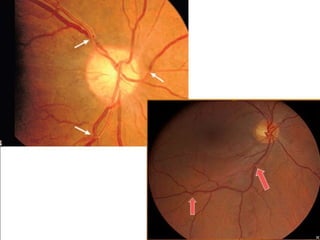
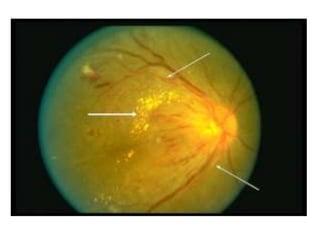
1. Hypertensive retinopathy refers to changes in the retina due to high blood pressure and includes narrowing of retinal arterioles, arteriovenous nicking, and hemorrhages.
2. It affects around 30% of people with hypertension. Major risk factors include age, family history, obesity, smoking, and stress.
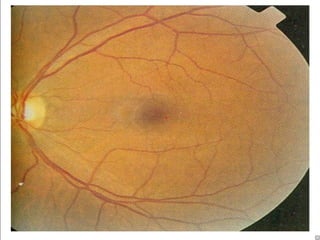
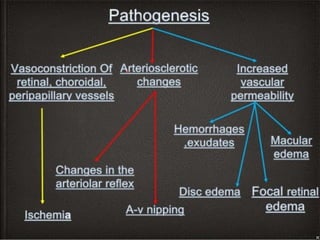
3. Changes are caused by vasoconstriction, arteriosclerotic changes, and increased vascular permeability from hypertension.
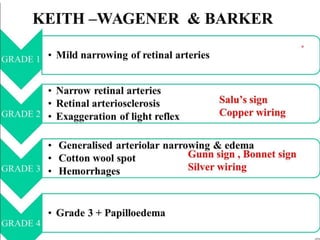
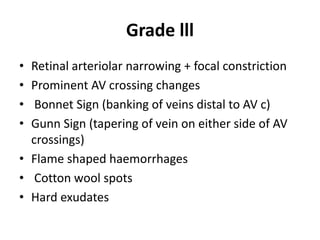
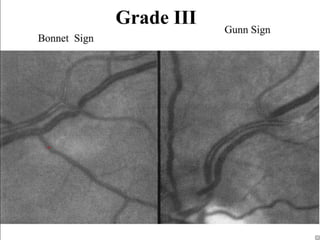
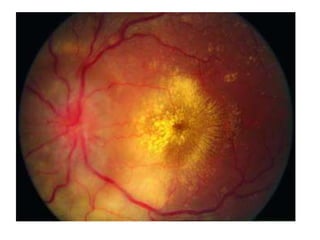
Hypertensive retinopathy is typically asymptomatic but some people experience blurry vision. Grading systems describe levels of changes from mild to severe involving hemorrhages, exudates, and optic disc swelling. Treatment focuses on blood